

Optimal Volume of the Residual Tumor to Predict Long-term Tumor Control Using Stereotactic Radiosurgery after Facial Nerve-preserving Surgery for Vestibular Schwannomas
- PMID: 33904259
- PMCID: PMC8076845
- DOI: 10.3346/jkms.2021.36.e102
Optimal Volume of the Residual Tumor to Predict Long-term Tumor Control Using Stereotactic Radiosurgery after Facial Nerve-preserving Surgery for Vestibular Schwannomas
Abstract
Background: Intended subtotal resection (STR) followed by adjuvant gamma knife radiosurgery (GKRS) has emerged as an effective treatment option for facial nerve (FN) preservation in vestibular schwannomas (VSs). This study aimed to identify the optimal cut-off volume of residual VS to predict favorable outcomes in terms of both tumor control and FN preservation.
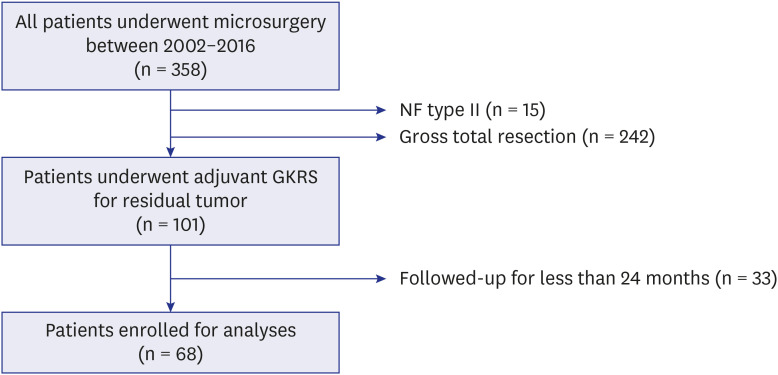
Methods: This retrospective study assessed the patients who underwent adjuvant GKRS for residual VS after microsurgery. A total of 68 patients who had been followed up for ≥ 24 months after GKRS were included. Tumor progression was defined as an increase in tumor volume (TV) of ≥ 20%. House-Brackmann grades I and II were considered to indicate good FN function.
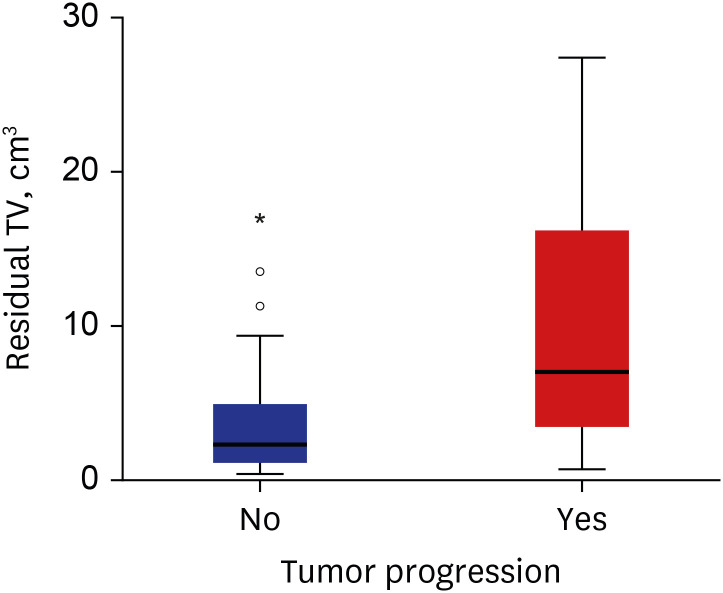
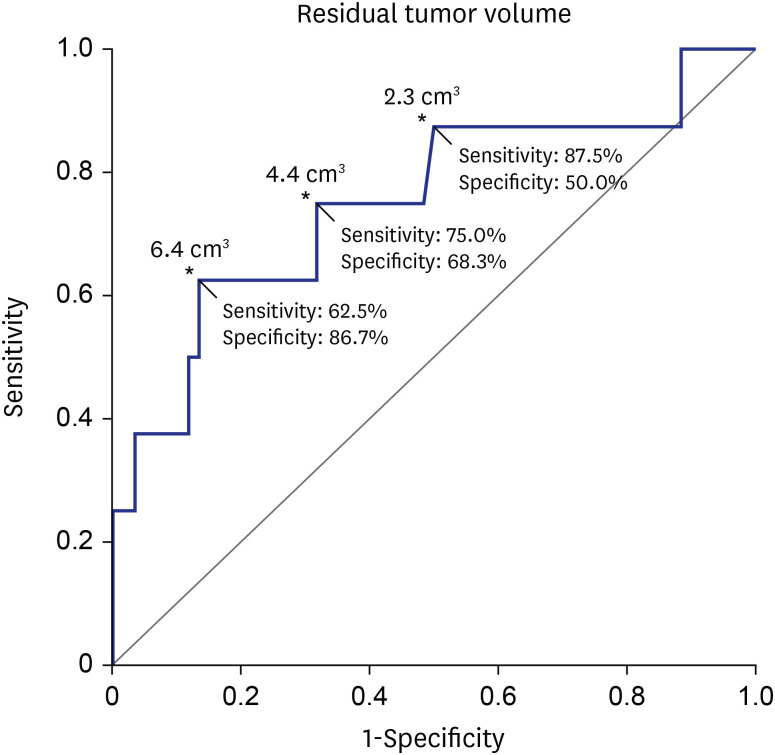
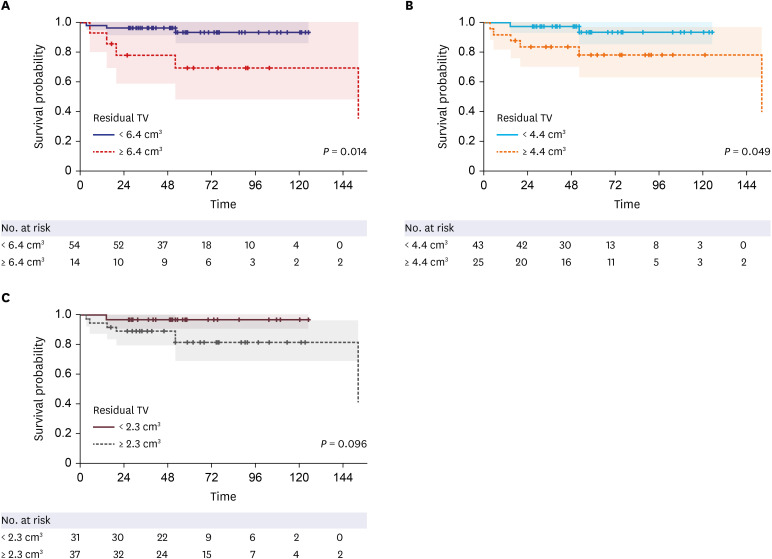
Results: The median residual TV was 2.5 cm³ (range: 0.3-27.4). The median follow-up period after the first adjuvant GKRS was 64 months (range: 25.7-152.4). Eight (12%) patients showed tumor progression. In multivariate analyses, residual TV was associated with tumor progression (P = 0.003; hazard ratio [HR], 1.229; 95% confidence interval [CI], 1.075-1.405). A residual TV of 6.4 cm³ was identified as the cut-off volume for showing the greatest difference in progression-free survival (PFS). The 5-year PFS rates in the group with residual TVs of < 6.4 cm³ (54 patients) and that with residual TVs of ≥ 6.4 cm³ (14 patients) were 93.3% and 69.3%, respectively (P = 0.014). A good FN outcome was achieved in 57 (84%) patients. Residual TV was not associated with good FN function during the immediate postoperative period (P = 0.695; odds ratio [OR], 1.024; 95% CI, 0.908-1.156) or at the last follow-up (P = 0.755; OR, 0.980; 95% CI, 0.866-1.110).
Conclusion: In this study, residual TV was associated with tumor progression in VS after adjuvant GKRS following STR. As preservation of FN function is not correlated with the extent of resection, optimal volume reduction is imperative to achieve long-term tumor control. Our findings will help surgeons predict the prognosis of residual VS after FN-preserving surgery.
Keywords: Facial Nerve; Gamma Knife Radiosurgery; Tumor Volume; Vestibular Schwannoma.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures

References
-
- Stangerup SE, Caye-Thomasen P. Epidemiology and natural history of vestibular schwannomas. Otolaryngol Clin North Am. 2012;45(2):257–268. - PubMed
-
- Betchen SA, Walsh J, Post KD. Self-assessed quality of life after acoustic neuroma surgery. J Neurosurg. 2003;99(5):818–823. - PubMed
-
- Bloch DC, Oghalai JS, Jackler RK, Osofsky M, Pitts LH. The fate of the tumor remnant after less-than-complete acoustic neuroma resection. Otolaryngol Head Neck Surg. 2004;130(1):104–112. - PubMed
-
- Chen Z, Prasad SC, Di Lella F, Medina M, Piccirillo E, Taibah A, et al. The behavior of residual tumors and facial nerve outcomes after incomplete excision of vestibular schwannomas. J Neurosurg. 2014;120(6):1278–1287. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
