

Physiological responses during ascent to high altitude and the incidence of acute mountain sickness
- PMID: 33904650
- PMCID: PMC8077104
- DOI: 10.14814/phy2.14809
Physiological responses during ascent to high altitude and the incidence of acute mountain sickness
Abstract
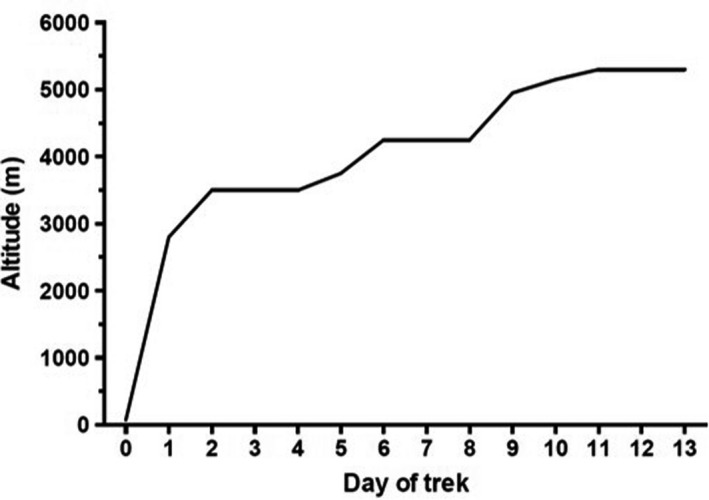
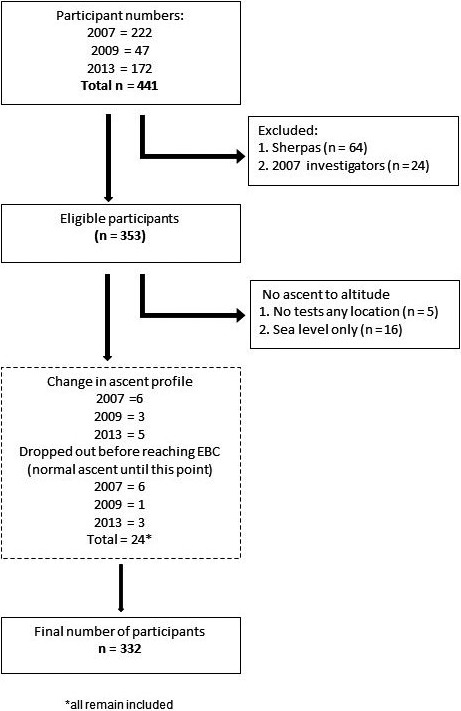
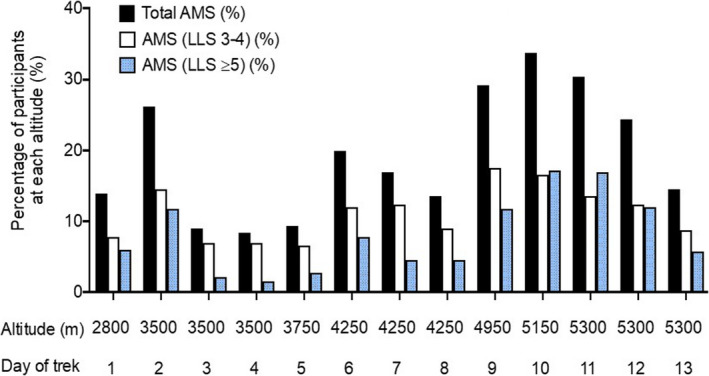
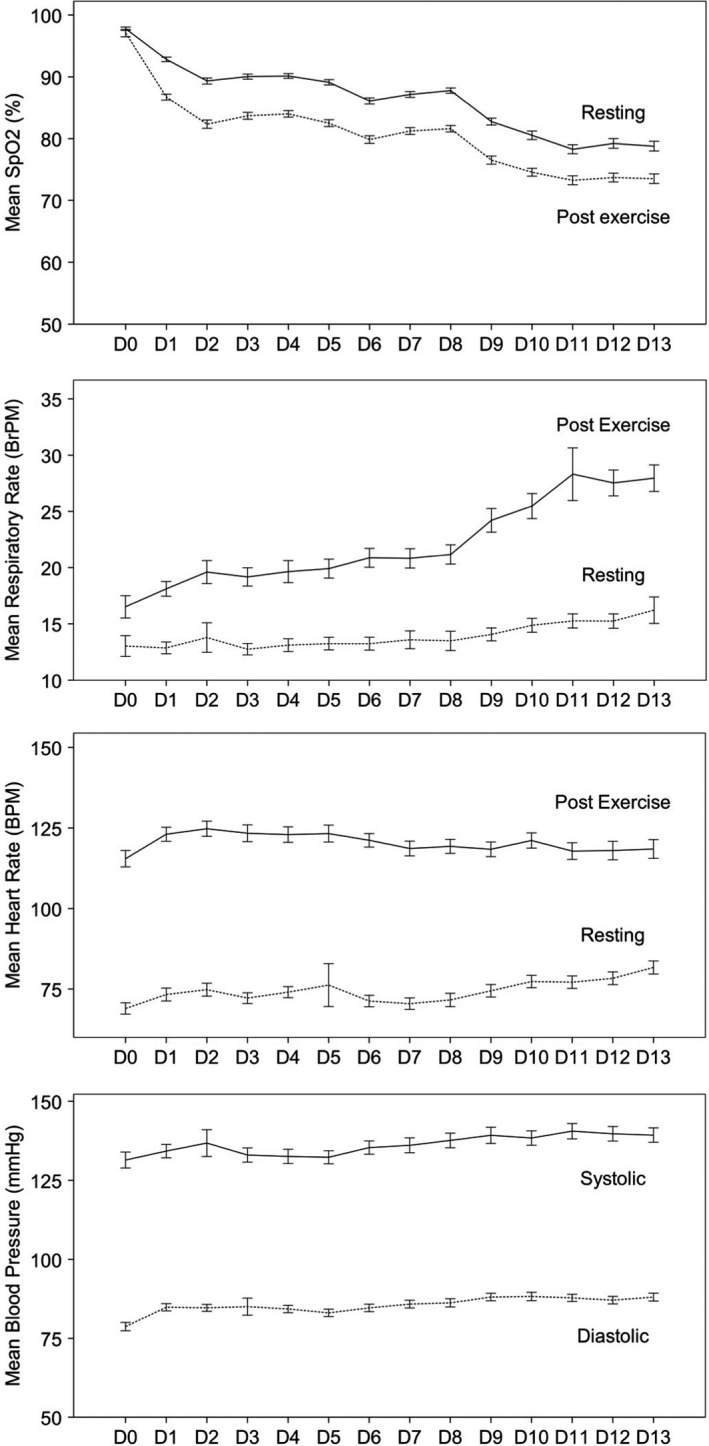
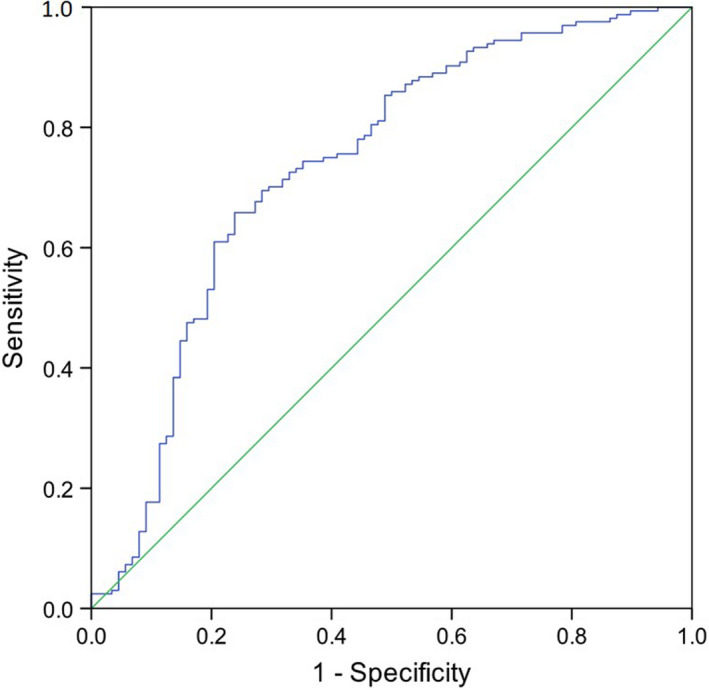
Acute mountain sickness (AMS) occurs when there is failure of acclimatisation to high altitude. The aim of this study was to describe the relationship between physiological variables and the incidence of AMS during ascent to 5300 m. A total of 332 lowland-dwelling volunteers followed an identical ascent profile on staggered treks. Self-reported symptoms of AMS were recorded daily using the Lake Louise score (mild 3-4; moderate-severe ≥5), alongside measurements of physiological variables (heart rate, respiratory rate (RR), peripheral oxygen saturation (SpO2 ) and blood pressure) before and after a standardised Xtreme Everest Step-Test (XEST). The overall occurrence of AMS among participants was 73.5% (23.2% mild, 50.3% moderate-severe). There was no difference in gender, age, previous AMS, weight or body mass index between participants who developed AMS and those who did not. Participants who had not previously ascended >5000 m were more likely to get moderate-to-severe AMS. Participants who suffered moderate-to-severe AMS had a lower resting SpO2 at 3500 m (88.5 vs. 89.6%, p = 0.02), while participants who suffered mild or moderate-to-severe AMS had a lower end-exercise SpO2 at 3500 m (82.2 vs. 83.8%, p = 0.027; 81.5 vs. 83.8%, p < 0.001 respectively). Participants who experienced mild AMS had lower end-exercise RR at 3500 m (19.2 vs. 21.3, p = 0.017). In a multi-variable regression model, only lower end-exercise SpO2 (OR 0.870, p < 0.001) and no previous exposure to altitude >5000 m (OR 2.740, p-value 0.003) predicted the development of moderate-to-severe AMS. The Xtreme Everest Step-Test offers a simple, reproducible field test to help predict AMS, albeit with relatively limited predictive precision.
Keywords: altitude; altitude sickness; exercise; hypoxia.
© 2021 The Authors. Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Figures
Comment in
-
A Step Test to Evaluate the Susceptibility to Severe High-Altitude Illness in Field Conditions.High Alt Med Biol. 2024 Sep;25(3):158-163. doi: 10.1089/ham.2023.0065. Epub 2024 Apr 29. High Alt Med Biol. 2024. PMID: 38682358
References
-
- Basnyat, B. , Lemaster, J. , & Litch, J. (1999). Everest or bust: a cross sectional, epidemiological study of acute mountain sickness at 4232 meters in the Himalayas. Aviation, Space & Environmental Medicine, 70, 867–873. - PubMed
-
- Burtscher, M. , Flatz, M. , & Faulhaber, M. (2004). Prediction of susceptibility to acute mountain sickness by SaO2 values during short‐term exposure to hypoxia. High Altitude Medicine & Biology, 5, 335–340. - PubMed
-
- Burtscher, M. , Szubski, C. , & Faulhaber, M. (2008). Prediction of the susceptibility to AMS in simulated altitude. Sleep and Breathing, 12, 103–108. - PubMed
-
- Chen, H. C. , Lin, W. L. , Wu, J. Y. , Wang, S. H. , Chiu, T. F. , Weng, Y. M. , Hsu, T. Y. , & Wu, M. H. (2012). Change in oxygen saturation does not predict acute mountain sickness on Jade Mountain. Wilderness & Environmental Medicine, 23, 122–127. - PubMed
-
- Faulhaber, M. , Wille, M. , Gatterer, H. , Heinrich, D. , & Burtscher, M. (2014). Resting arterial oxygen saturation and breathing frequency as predictors for acute mountain sickness development: A prospective cohort study. Sleep and Breathing, 18, 669–674. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
