

Hospital Quality Improvement Interventions, Statewide Policy Initiatives, and Rates of Cesarean Delivery for Nulliparous, Term, Singleton, Vertex Births in California
- PMID: 33904868
- PMCID: PMC8080226
- DOI: 10.1001/jama.2021.3816
Hospital Quality Improvement Interventions, Statewide Policy Initiatives, and Rates of Cesarean Delivery for Nulliparous, Term, Singleton, Vertex Births in California
Abstract
Importance: Safe reduction of the cesarean delivery rate is a national priority.
Objective: To evaluate the rates of cesarean delivery for nulliparous, term, singleton, vertex (NTSV) births in California in the context of a statewide multifaceted intervention designed to reduce the rates of cesarean delivery.
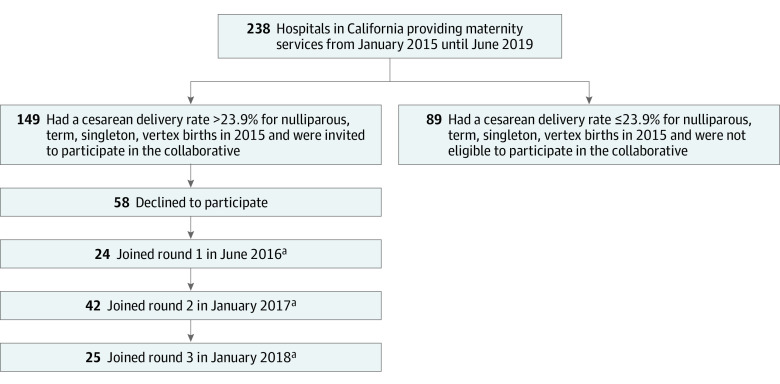
Design, setting, and participants: Observational study of cesarean delivery rates from 2014 to 2019 among 7 574 889 NTSV births in the US and at 238 nonmilitary hospitals providing maternity services in California. From 2016 to 2019, California Maternal Quality Care Collaborative partnered with Smart Care California to implement multiple approaches to decrease the rates of cesarean delivery. Hospitals with rates of cesarean delivery greater than 23.9% for NTSV births were invited to join 1 of 3 cohorts for an 18-month quality improvement collaborative between July 2016 and June 2019.
Exposures: Within the collaborative, multidisciplinary teams implemented multiple strategies supported by mentorship, shared learning, and rapid-cycle data feedback. Partnerships among nonprofit organizations, state governmental agencies, purchasers, and health plans addressed the external environment through transparency, award programs, and incentives.
Main outcomes and measures: The primary outcome was the change in cesarean delivery rates for NTSV births in California and a difference-in-differences analysis was performed to compare cesarean delivery rates for NTSV births in California vs the rates in the rest of the US. A mixed multivariable logistic regression model that adjusted for patient-level and hospital-level confounders also was used to assess the collaborative and the external statewide actions. The cesarean delivery rates for NTSV births at hospitals participating in the collaborative were compared with the rates from the nonparticipating hospitals and the rates in the participating hospitals prior to participation in the collaborative.
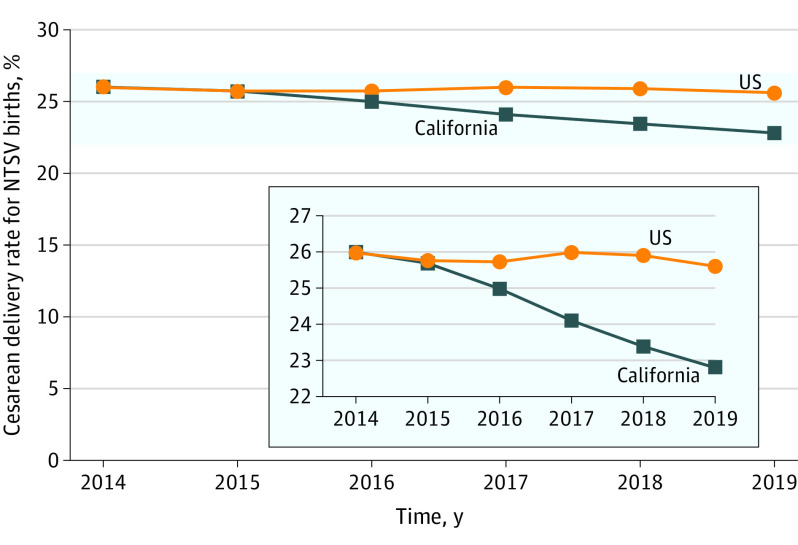
Results: A total of 7 574 889 NTSV births occurred in the US from 2014 to 2019, of which 914 283 were at 238 hospitals in California. All California hospitals were exposed to the statewide actions to reduce the rates of cesarean delivery, including the 149 hospitals that had baseline rates of cesarean delivery greater than 23.9% for NTSV births, of which 91 (61%) participated in the quality improvement collaborative. The rate of cesarean delivery for NTSV births in California decreased from 26.0% (95% CI, 25.8%-26.2%) in 2014 to 22.8% (95% CI, 22.6%-23.1%) in 2019 (relative risk, 0.88; 95% CI, 0.87-0.89). The rate of cesarean delivery for NTSV births in the US (excluding California births) was 26.0% in both 2014 and 2019 (relative risk, 1.00; 95% CI, 0.996-1.005). The difference-in-differences analysis revealed that the reduction in the rate of cesarean delivery for NTSV births in California was 3.2% (95% CI, 1.7%-3.5%) higher than in the US (excluding California). Compared with the hospitals and the periods not exposed to the collaborative activities, and after adjusting for patient characteristics and time using a modified stepped-wedge analysis, exposure to collaborative activities was associated with a lower odds of cesarean delivery for NTSV births (24.4% vs 24.6%; adjusted odds ratio, 0.87 [95% CI, 0.85-0.89]).
Conclusions and relevance: In this observational study of NTSV births in California from 2014 to 2019, the rates of cesarean delivery decreased over time in the setting of the implementation of a coordinated hospital-level collaborative and statewide initiatives designed to support vaginal birth.
Conflict of interest statement
Figures
Comment in
-
Initiatives to Reduce Cesarean Delivery Rates for Low-risk First Births.JAMA. 2021 Apr 27;325(16):1616-1617. doi: 10.1001/jama.2021.0084. JAMA. 2021. PMID: 33904887 No abstract available.
References
-
- Main EK, Morton CH, Melsop K, et al. Creating a public agenda for maternity safety and quality in cesarean delivery. Obstet Gynecol. 2012;120(5):1194-1198. - PubMed
-
- Office of Disease Prevention and Health Promotion . Healthy People 2020: topics and objectives, maternal, infant, and child health. Accessed August 26, 2020. https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infa...
-
- National Center for Health Statistics . Chapter 26: Maternal, infant, and child health. In: Healthy People 2020 Midcourse Review. National Center for Health Statistics; 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
