

Carotid stiffness is associated with retinal microvascular dysfunction-The Maastricht study
- PMID: 33905576
- PMCID: PMC8459287
- DOI: 10.1111/micc.12702
Carotid stiffness is associated with retinal microvascular dysfunction-The Maastricht study
Abstract
Objective: This study investigated whether arterial stiffening is a determinant of subtle retinal microvascular changes that precede diabetic retinopathy.
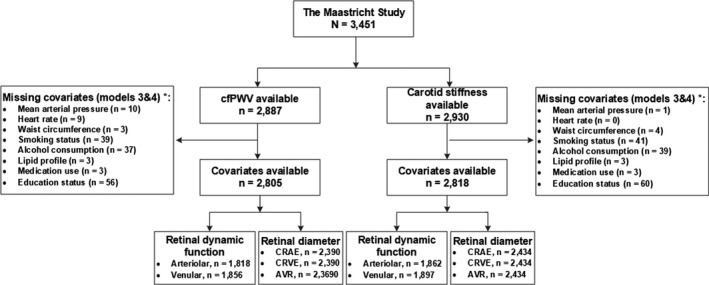
Research design and methods: This study used cross-sectional data from the Maastricht Study, a type 2 diabetes-enriched population-based cohort study. We used multivariable linear regression analysis to investigate, in individuals without and with type 2 diabetes, the associations of carotid distensibility coefficient and carotid-femoral pulse wave velocity with retinal microvascular diameters and flicker light-induced dilation and adjusted for cardiovascular and lifestyle risk factors.
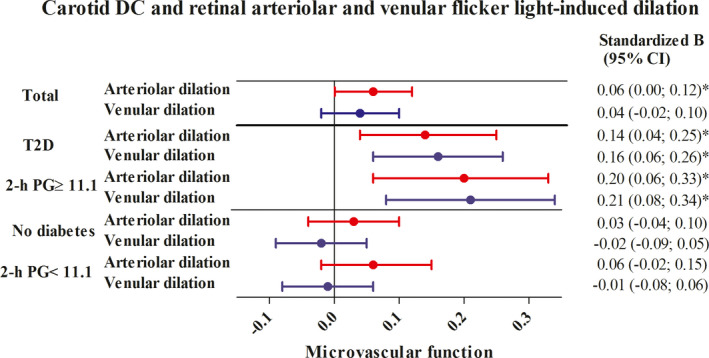
Results: The retinal microvascular diameter study population consisted of N = 2434 participants (51.4% men, mean ± SD age 59.8 ± 8.1 years, and 28.1% type 2 diabetes). No measures of arterial stiffness were significantly associated with microvascular diameters. Greater carotid distensibility coefficient (i.e., lower carotid stiffness) was significantly associated with greater retinal arteriolar flicker light-induced dilation (per standard deviation, standardized beta [95% CI] 0.06 [0.00; 0.12]) and non-significantly, but directionally similarly, associated with greater retinal venular flicker light-induced dilation (0.04 [-0.02; 0.10]). Carotid-femoral pulse wave velocity (i.e., aortic stiffness) was not associated with retinal microvascular flicker light-induced dilation. The associations between carotid distensibility coefficient and retinal arteriolar and venular flicker light-induced dilation were two- to threefold stronger in individuals with type 2 diabetes than in those without.
Conclusion: In this population-based study greater carotid, but not aortic, stiffness was associated with worse retinal flicker light-induced dilation and this association was stronger in individuals with type 2 diabetes. Hence, carotid stiffness may be a determinant of retinal microvascular dysfunction.
Keywords: aortic stiffness; arterial stiffness; carotid stiffness; diabetic retinopathy; microvascular dysfunction; retinal microvascular diameter; type 2 diabetes mellitus.
© 2021 The Authors. Microcirculation published by John Wiley & Sons Ltd.
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported.
Figures
References
-
- Stehouwer CDA. Microvascular dysfunction and hyperglycemia: a vicious cycle with widespread consequences. Diabetes. 2018;67:1729‐1741. - PubMed
-
- Lim M, Sasongko MB, Ikram MK, et al. Systemic associations of dynamic retinal vessel analysis: a review of current literature. Microcirculation. 2013;20:257‐268. - PubMed
-
- de Clerck EEB, Schouten JSAG, Berendschot TTJM, et al. Loss of temporal peripapillary retinal nerve fibers in prediabetes or type 2 diabetes without diabetic retinopathy: the Maastricht study. Invest Ophthalmol Vis Sci. 2017;58:1017‐1027.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
