

Demand for Essential Nonambulatory Neurosurgical Care Decreased While Acuity of Care Increased During the Coronavirus Disease 2019 (COVID-19) Surge
- PMID: 33905912
- PMCID: PMC8589108
- DOI: 10.1016/j.wneu.2021.04.080
Demand for Essential Nonambulatory Neurosurgical Care Decreased While Acuity of Care Increased During the Coronavirus Disease 2019 (COVID-19) Surge
Abstract
Background: In times of health resource reallocation, capacities must remain able to meet a continued demand for essential, nonambulatory neurosurgical acute care. This study sought to characterize the demand for and provision of neurosurgical acute care during the coronavirus disease 2019 (COVID-19) pandemic.
Methods: This single-center cross-sectional observational analysis compared nonambulatory neurosurgical consult encounters during the peri-surge period (March 9 to May 31, 2020) with those during an analogous period in 2019. Outcomes included consult volume, distribution of problem types, disease severity, and rate of acute operative intervention.
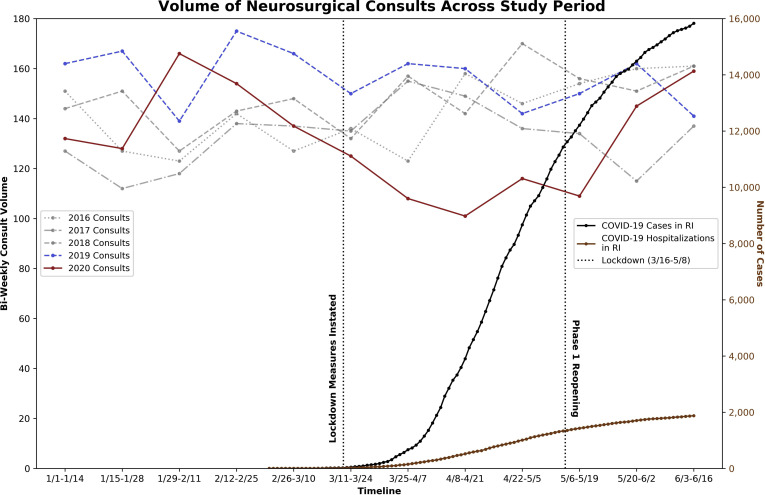
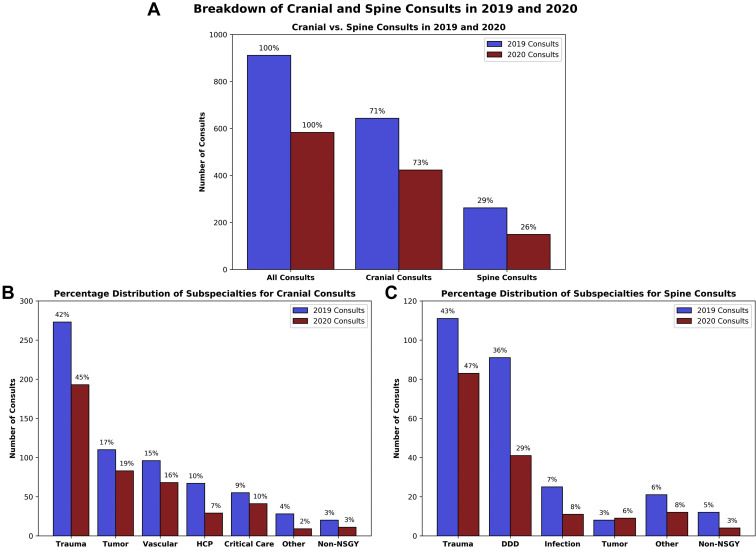
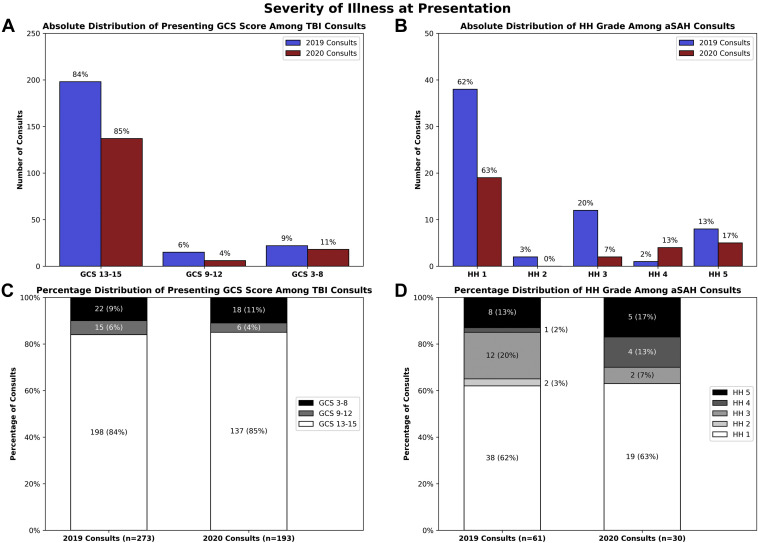
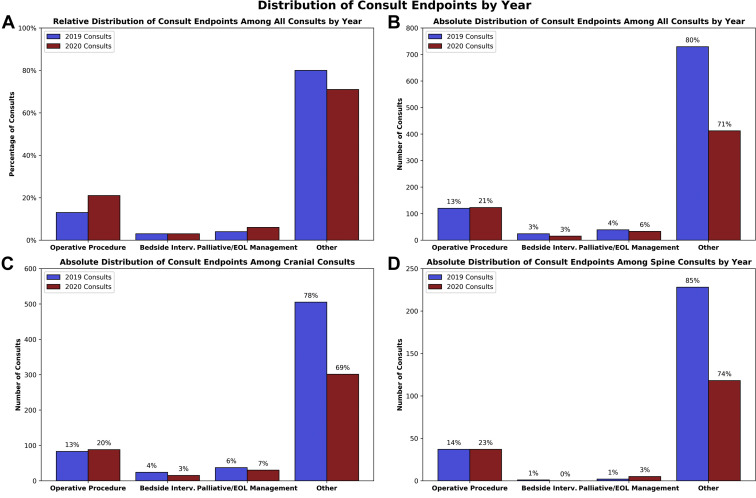
Results: A total of 1494 neurosurgical consults were analyzed. Amidst the pandemic surge, 583 consults were seen, which was 6.4 standard deviations below the mean among analogous 2016-2019 periods (mean 873; standard deviation 45, P = 0.001). Between 2019 and 2020, the proportion of degenerative spine consults decreased in favor of spinal trauma (25.6% vs. 34% and 51.9% vs. 41.4%, P = 0.088). Among aneurysmal subarachnoid hemorrhage cases, poor-grade (Hunt and Hess grades 4-5) presentations were more common (30% vs. 14.8%, P = 0.086). A greater proportion of pandemic era consults resulted in acute operative management, with an unchanged absolute frequency of acutely operative consults (123/583 [21.1%] vs. 120/911 [13.2%], P < 0.001).
Conclusions: Neurosurgical consult volume during the pandemic surge hit a 5-year institutional low. Amidst vast reallocation of health care resources, demand for high-acuity nonambulatory neurosurgical care continued and proportionally increased for greater-acuity pathologies. In our continued current pandemic as well as any future situations of mass health resource reallocation, neurosurgical acute care capacities must be preserved.
Keywords: Acute care neurosurgery; COVID-19 surge; Pandemic preparedness; Public health.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Neurosurgical Outcomes, Protocols, and Resource Management During Lockdown: Early Institutional Experience from One of the World's Largest COVID 19 Hotspots.World Neurosurg. 2021 Nov;155:e34-e40. doi: 10.1016/j.wneu.2021.07.082. Epub 2021 Jul 26. World Neurosurg. 2021. PMID: 34325030 Free PMC article.
-
Neurosurgery Subspecialty Practice During a Pandemic: A Multicenter Analysis of Operative Practice in 7 U.S. Neurosurgery Departments During Coronavirus Disease 2019.World Neurosurg. 2022 Sep;165:e242-e250. doi: 10.1016/j.wneu.2022.06.010. Epub 2022 Jun 18. World Neurosurg. 2022. PMID: 35724884 Free PMC article.
-
A snapshot of European neurosurgery December 2019 vs. March 2020: just before and during the Covid-19 pandemic.Acta Neurochir (Wien). 2020 Sep;162(9):2221-2233. doi: 10.1007/s00701-020-04482-8. Epub 2020 Jul 8. Acta Neurochir (Wien). 2020. PMID: 32642834 Free PMC article.
-
Early Responses of Neurosurgical Practice to the Coronavirus Disease 2019 (COVID-19) Pandemic: A Rapid Review.World Neurosurg. 2020 Sep;141:e1017-e1026. doi: 10.1016/j.wneu.2020.06.167. Epub 2020 Jun 26. World Neurosurg. 2020. PMID: 32599184 Free PMC article.
-
Reconversion of neurosurgical practice in times of the SARS-CoV-2 pandemic: a narrative review of the literature and guideline implementation in a Mexican neurosurgical referral center.Neurosurg Focus. 2020 Dec;49(6):E4. doi: 10.3171/2020.9.FOCUS20553. Neurosurg Focus. 2020. PMID: 33260129 Review.
Cited by
-
Letter to the Editor Regarding "Viscoelastic Hemostatic Assays and Outcomes in Traumatic Brain Injury: A Systematic Literature Review".World Neurosurg. 2022 Oct;166:291-293. doi: 10.1016/j.wneu.2022.04.040. World Neurosurg. 2022. PMID: 36192854 Free PMC article. No abstract available.
References
-
- Fineberg H.V. The toll of COVID-19. JAMA. 2020;324:1502–1503. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
