

Sacrococcygeal Teratoma : A Tumor at the Center of Embryogenesis
- PMID: 33906346
- PMCID: PMC8128526
- DOI: 10.3340/jkns.2021.0015
Sacrococcygeal Teratoma : A Tumor at the Center of Embryogenesis
Abstract
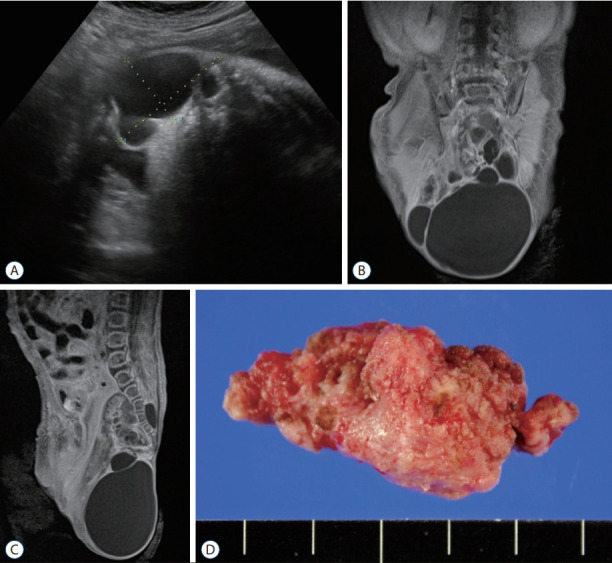
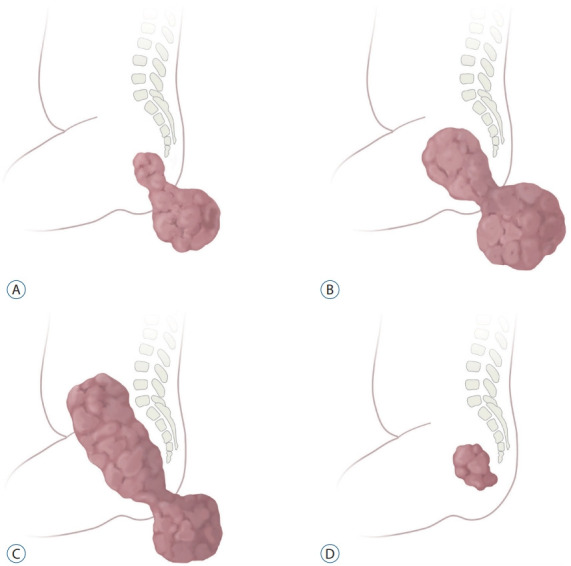
Sacrococcygeal teratoma (SCT) is an extragonadal germ cell tumor (GCT) that develops in the fetal and neonatal periods. SCT is a type I GCT in which only teratoma and yolk sac tumors arise from extragonadal sites. SCT is the most common type I GCT and is believed to originate through epigenetic reprogramming of early primordial germ cells migrating from the yolk sac to the gonadal ridges. Fetal SCT diagnosed in utero presents many obstetrical problems. For high-risk fetuses, fetal interventions (devascularization and debulking) are under development. Most patients with SCT are operated on after birth. Complete surgical resection is the key for tumor control, and the anatomical location of the tumor determines the surgical approaches. Incomplete resection and malignant histology are risk factors for recurrence. Approximately 10-15% of patients have a tumor recurrence, which is frequently of malignant histology. Long-term surveillance with monitoring of serum alpha fetoprotein and magnetic resonance imaging is required. Survivors of SCT may suffer anorectal, urological, and sexual sequelae later in their life, and comprehensive evaluation and care are required.
Keywords: Fetus; Germ cell tumor; Surgery; Teratoma, Sacrococcygeal.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Altman RP, Randolph JG, Lilly JR. Sacrococcygeal teratoma: American academy of pediatrics surgical section survey-1973. J Pediatr Surg. 1974;9:389–398. - PubMed
-
- Anteby EY, Yagel S. Route of delivery of fetuses with structural anomalies. Eur J Obstet Gynecol Reprod Biol. 2003;106:5–9. - PubMed
-
- Bader D, Riskin A, Vafsi O, Tamir A, Peskin B, Israel N, et al. Alphafetoprotein in the early neonatal period--a large study and review of the literature. Clin Chim Acta. 2004;349:15–23. - PubMed
-
- Barksdale EM, Jr, Obokhare I. Teratomas in infants and children. Curr Opin Pediatr. 2009;21:344–349. - PubMed
-
- Cowles RA, Stolar CJ, Kandel JJ, Weintraub JL, Susman J, Spigland NA. Preoperative angiography with embolization and radiofrequency ablation as novel adjuncts to safe surgical resection of a large, vascular sacrococcygeal teratoma. Pediatr Surg Int. 2006;22:554–556. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
