

Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile
- PMID: 33906968
- PMCID: PMC8158961
- DOI: 10.1126/science.abg5298
Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile
Abstract
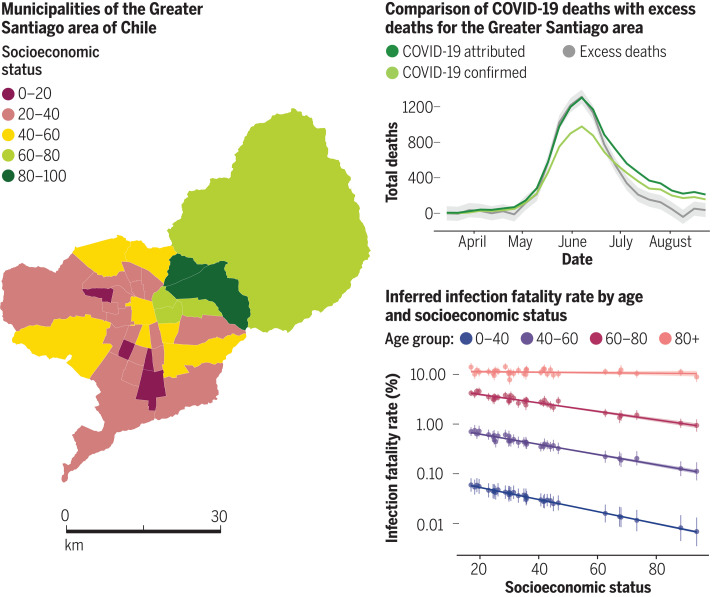
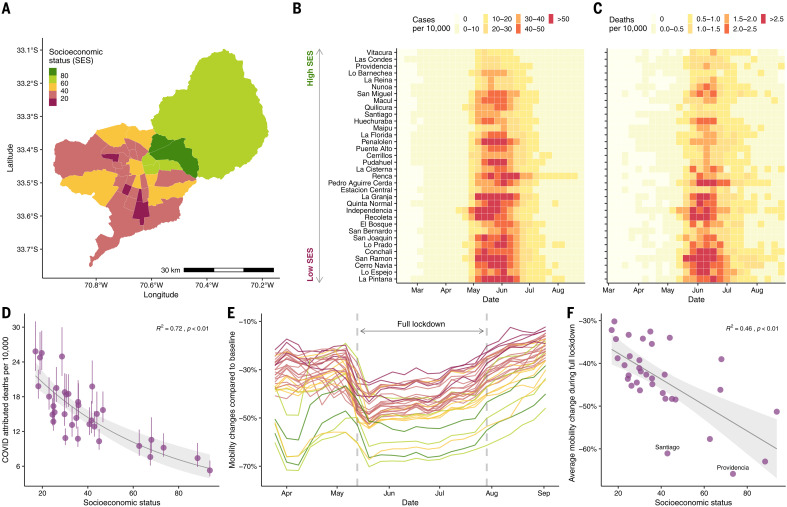
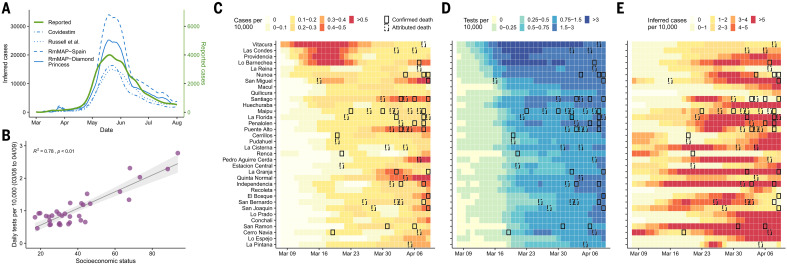
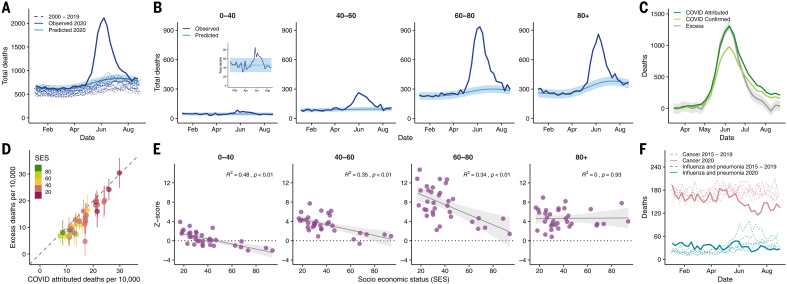
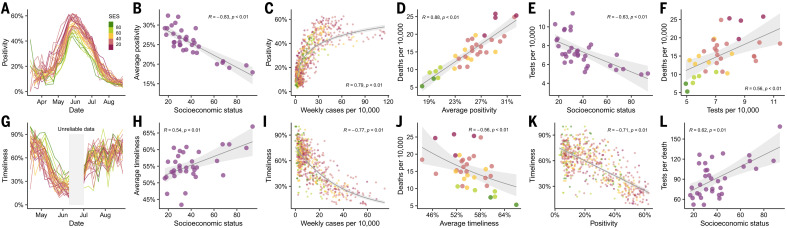
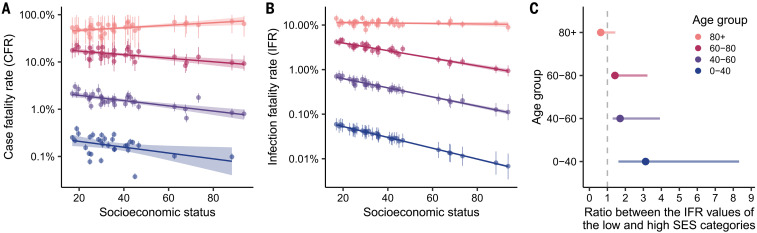
The COVID-19 pandemic has affected cities particularly hard. Here, we provide an in-depth characterization of disease incidence and mortality and their dependence on demographic and socioeconomic strata in Santiago, a highly segregated city and the capital of Chile. Our analyses show a strong association between socioeconomic status and both COVID-19 outcomes and public health capacity. People living in municipalities with low socioeconomic status did not reduce their mobility during lockdowns as much as those in more affluent municipalities. Testing volumes may have been insufficient early in the pandemic in those places, and both test positivity rates and testing delays were much higher. We find a strong association between socioeconomic status and mortality, measured by either COVID-19-attributed deaths or excess deaths. Finally, we show that infection fatality rates in young people are higher in low-income municipalities. Together, these results highlight the critical consequences of socioeconomic inequalities on health outcomes.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Update of
-
Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile.medRxiv [Preprint]. 2021 Jan 15:2021.01.12.21249682. doi: 10.1101/2021.01.12.21249682. medRxiv. 2021. Update in: Science. 2021 May 28;372(6545):eabg5298. doi: 10.1126/science.abg5298. PMID: 33469598 Free PMC article. Updated. Preprint.
Comment in
-
Universal health care must be a priority - even amid COVID.Nature. 2021 May;593(7859):313-314. doi: 10.1038/d41586-021-01313-3. Nature. 2021. PMID: 34007078 No abstract available.
References
-
- Kraemer M. U. G., Yang C.-H., Gutierrez B., Wu C.-H., Klein B., Pigott D. M., du Plessis L., Faria N. R., Li R., Hanage W. P., Brownstein J. S., Layan M., Vespignani A., Tian H., Dye C., Pybus O. G., Scarpino S. V., Open COVID-19 Data Working Group , The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 368, 493–497 (2020). 10.1126/science.abb4218 - DOI - PMC - PubMed
-
- Pullano G., Valdano E., Scarpa N., Rubrichi S., Colizza V., Evaluating the effect of demographic factors, socioeconomic factors, and risk aversion on mobility during the COVID-19 epidemic in France under lockdown: A population-based study. The Lancet Digital Health 2, e638–e649 (2020). 10.1016/S2589-7500(20)30243-0 - DOI - PMC - PubMed
-
- Chinazzi M., Davis J. T., Ajelli M., Gioannini C., Litvinova M., Merler S., Pastore Y Piontti A., Mu K., Rossi L., Sun K., Viboud C., Xiong X., Yu H., Halloran M. E., Longini I. M. Jr.., Vespignani A., The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 368, 395–400 (2020). 10.1126/science.aba9757 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
