

Comparison of the efficacy and safety of subthreshold micropulse laser with photodynamic therapy for the treatment of chronic central serous chorioretinopathy: A meta-analysis
- PMID: 33907163
- PMCID: PMC8084005
- DOI: 10.1097/MD.0000000000025722
Comparison of the efficacy and safety of subthreshold micropulse laser with photodynamic therapy for the treatment of chronic central serous chorioretinopathy: A meta-analysis
Abstract
Background: This meta-analysis was conducted to compare the therapeutic effect and safety of subthreshold micropulse laser (SML) vs photodynamic therapy (PDT) in treatment of chronic central serous chorioretinopathy (cCSC).
Methods: PubMed, EMBASE, and the Cochrane Library were searched for all relevant studies published up to August 17, 2020. Data of interest were analyzed by STATA (version 14.0) software.
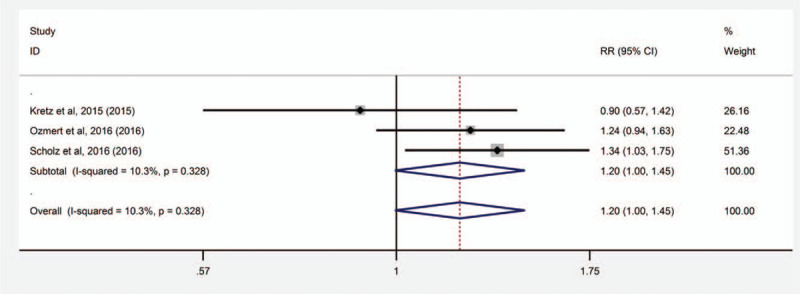
Results: Four randomized clinical trials (RCTs) and 5 retrospective studies with 790 eyes were included in this meta-analysis after study selection. The results showed that SML significantly improved the best-corrected visual acuity (BCVA) compared with PDT at 6 to 8 weeks, 6 months, and 7 to 8 months in patients with cCSC (weighted mean difference (WMD) = -0.15, 95% confidence intervals (CI): -0.23 to -0.07, P < .01; WMD = -2.83, 95% CI: -4.79 to -0.87, P < .01; and WMD = -2.61, 95% CI: -4.23 to -1.24, P = .026, respectively). There was also a statistically significant difference between SML and PDT groups in the differences in the complete resolution of subretinal fluid (SRF) (risk radios = 0.388, 95% CI: 0.307 to 0.491, P < .01). There were no significant differences between the SML and PDT in the overall effect with central macular thickness (CMT), adverse events, complete resolution of SRF and treatment response.
Conclusions: Based on the available evidence, this meta-analysis demonstrated that SML may be considered as a competitive alternative to PDT for treating cCSC, and as the first-line treatment of cCSC.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interests to disclose.
Figures







References
-
- Spaide RF, Campeas L, Haas A, et al. . Central serous chorioretinopathy in younger and older adults. Ophthalmology 1996;103:2070–80. - PubMed
-
- Gemenetzi M, De Salvo G, Lotery AJ. Central serous chorioretinopathy: an update on pathogenesis and treatment. Eye 2010;24:1743–56. - PubMed
-
- Ross A, Ross AH, Mohamed Q. Review and update of central serous chorioretinopathy. Curr Opin Ophthalmol 2011;22:166–73. - PubMed
-
- PRüNTE C, Flammer J. Choroidal capillary and venous congestion in central serous chorioretinopathy. Am J Ophthalmol 1996;121:26–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
