

Association of blood biomarkers and autoimmunity with immune related adverse events in patients with cancer treated with immune checkpoint inhibitors
- PMID: 33907229
- PMCID: PMC8079370
- DOI: 10.1038/s41598-021-88307-3
Association of blood biomarkers and autoimmunity with immune related adverse events in patients with cancer treated with immune checkpoint inhibitors
Abstract
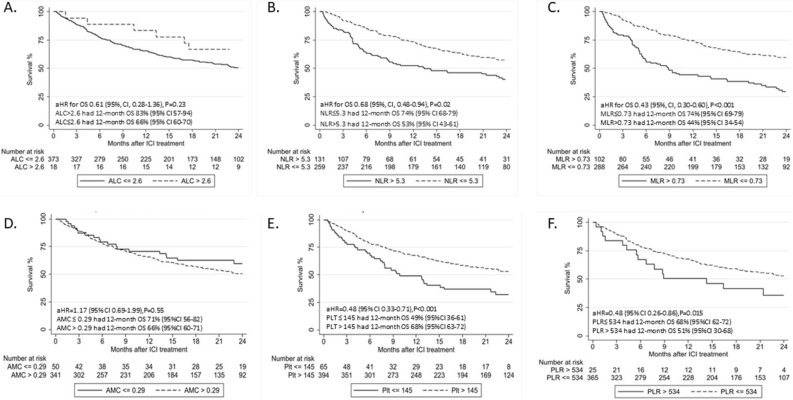
Patients with cancer treated with immune checkpoint inhibitors (ICIs) develop immune related adverse events (irAEs), however biomarkers are lacking. We hypothesized that clinicopathologic and laboratory factors would be associated with irAE risk and overall survival (OS) in this population. In a retrospective study of patients treated with ICIs we collected clinicopathologic, laboratory, irAEs and outcomes data. The association between baseline blood biomarkers, clinicopathologic features and irAEs was assessed by logistic regression adjusting for age, sex, smoking, cancer type, performance status, concomitant other systemic therapy, history of autoimmune disease (AD), chronic infection and pre-existing systemic steroid use (regardless of dose). Optimal cutoff values of biomarkers were identified by recursive partitioning analysis. 470 patients were identified; 156 (33%) developed irAEs, which were associated with baseline absolute lymphocyte count > 2.6 k/ul (adjusted [a]OR: 4.30), absolute monocyte count > 0.29 k/ul (aOR: 2.34) and platelet count > 145 k/ul (aOR: 2.23), neutrophil to lymphocyte ratio (NLR) ≤ 5.3 (aOR: 2.07) and monocyte to lymphocyte ratio (MLR) ≤ 0.73 (aOR: 2.96), as well as platelet to lymphocyte ratio ≤ 534 (aOR: 5.05). Patients with pre-existing AD (aOR: 2.57), family history of AD (aOR: 5.98), and ICI combination (aOR: 2.00) had higher odds of irAEs. Baseline NLR ≤ 5.3 (aHR: 0.68), MLR ≤ 0.73 (aHR: 0.43), PLT > 145 (aHR: 0.48) and PLR ≤ 534 (aHR: 0.48) were associated with longer OS. irAEs were associated with autoimmune history, ICI combination and baseline laboratory measurements. Lower NLR, MLR and PLR may have favorable prognostic value. Our hypothesis-generating findings require validation in larger prospective studies.
Conflict of interest statement
Dr. D Michailidou has no disclosures. Dr. AR Khaki: owned stock from Merck and Sanofi within the last 3 years. Dr. MP Morelli has not disclosures. Dr. L Diamantopoulos has no disclosures. Dr. N Singh has no disclosures. Dr. P Grivas (all unrelated in the last 3 years): Consulting: AstraZeneca; Bayer; Bristol-Myers Squibb; Clovis Oncology; Dyania Health, Driver; EMD Serono; Exelixis; Foundation Medicine; Genentech/Roche; Genzyme; GlaxoSmithKline; Heron Therapeutics; Immunomedics, Infinity Pharmaceuticals; Janssen; Merck; Mirati Therapeutics; Pfizer; Seattle Genetics; QED Therapeutics. Research Funding to Institution: Merck; Pfizer, Clovis Oncology, Bavarian Nordic, Immunomedics, Debiopharm, Bristol-Myers Squibb, QED Therapeutics, GlaxoSmithKline, Mirati Therapeutics, Kure It Cancer Research.
Figures
References
-
- Kumar P, et al. Cancer immunotherapy with checkpoint inhibitor can cause autoimmune adverse events due to loss of Treg homeostasis. Semin. Cancer Biol. (2019). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
