

Optimal Timing of Radiotherapy after Incomplete Transarterial Chemoembolization for Barcelona Clinic Liver Cancer Stage B Hepatocellular Carcinoma
- PMID: 33908211
- PMCID: PMC8084693
- DOI: 10.3349/ymj.2021.62.5.409
Optimal Timing of Radiotherapy after Incomplete Transarterial Chemoembolization for Barcelona Clinic Liver Cancer Stage B Hepatocellular Carcinoma
Abstract
Purpose: The optimal timing for radiotherapy (RT) after incomplete transarterial chemoembolization (TACE) remains unclear. This study investigated the optimal timing to initiate RT after incomplete TACE in patients with Barcelona Clinic Liver Cancer stage B hepatocellular carcinoma.
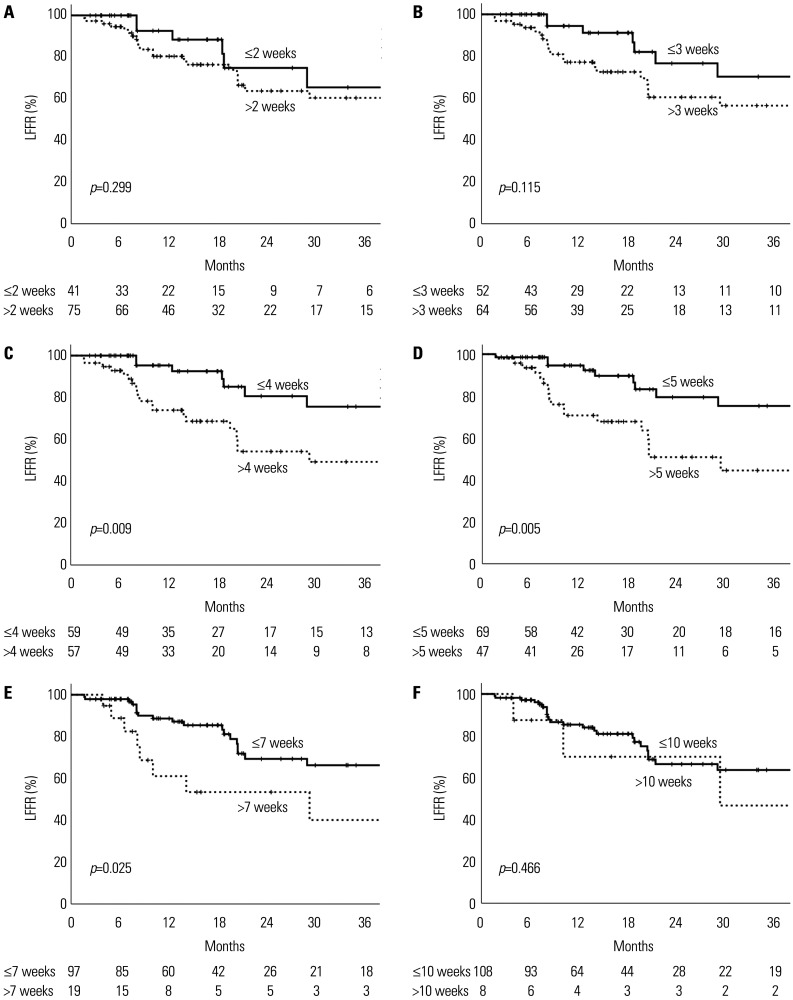
Materials and methods: This study included 116 lesions in 104 patients who were treated with RT after TACE between 2001 and 2016. The time interval between the last TACE session and RT initiation was retrospectively analyzed. The optimal cut-off time interval that maximized the difference in local failure-free rates (LFFRs) was determined using maximally selected rank statistics.
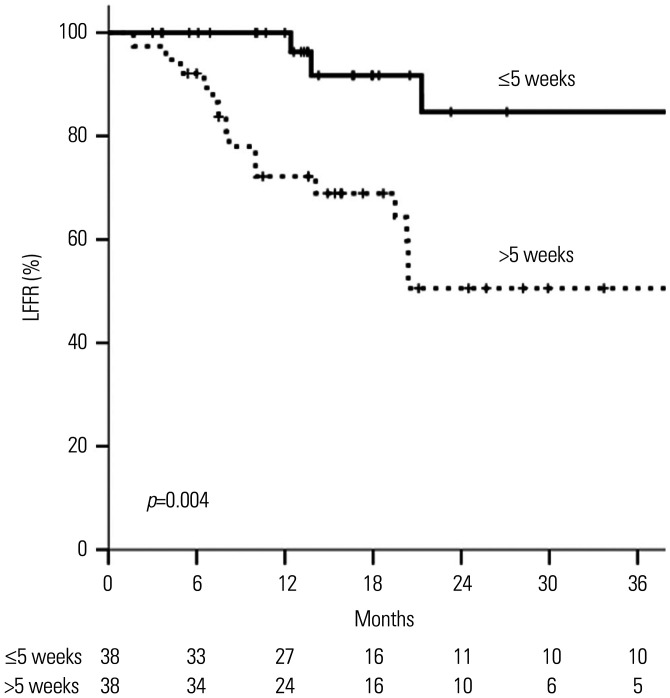
Results: The median time interval was 26 days (range: 2-165 days). At a median follow-up of 18 months (range: 3-160 months), the median overall survival was 18 months. The optimal cut-off time interval appeared to be 5 weeks; using this cut-off, 65 and 39 patients were classified into early and late RT groups, respectively. Early RT group had a significantly poorer Child-Pugh class and higher alpha-fetoprotein levels compared to late RT group. Other characteristics, including tumor size (7 cm vs. 6 cm; p=0.144), were not significantly different between the groups. The 1-year LFFR was significantly higher in the early RT group than in the late RT group (94.6% vs. 70.8%; p=0.005). On multivariate analysis, early RT was identified as an independent predictor of favorable local failure-free survival (hazard ratio: 3.30, 95% confidence interval: 1.50-7.29; p=0.003).
Conclusion: The optimal timing for administering RT after incomplete TACE is within 5 weeks. Early administration of RT is associated with better local control.
Keywords: Carcinoma, hepatocellular; chemoembolization, therapeutic; radiotherapy.
© Copyright: Yonsei University College of Medicine 2021.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures


References
-
- Higuchi T, Kikuchi M, Okazaki M. Hepatocellular carcinoma after transcatheter hepatic arterial embolization. A histopathologic study of 84 resected cases. Cancer. 1994;73:2259–2267. - PubMed
-
- Wang B, Xu H, Gao ZQ, Ning HF, Sun YQ, Cao GW. Increased expression of vascular endothelial growth factor in hepatocellular carcinoma after transcatheter arterial chemoembolization. Acta Radiol. 2008;49:523–529. - PubMed
-
- Huo YR, Eslick GD. Transcatheter arterial chemoembolization plus radiotherapy compared with chemoembolization alone for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Oncol. 2015;1:756–765. - PubMed
-
- Choi C, Koom WS, Kim TH, Yoon SM, Kim JH, Lee HS, et al. A prospective phase 2 multicenter study for the efficacy of radiation therapy following incomplete transarterial chemoembolization in unresectable hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2014;90:1051–1060. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
