

Assessment of Catheter Ablation or Antiarrhythmic Drugs for First-line Therapy of Atrial Fibrillation: A Meta-analysis of Randomized Clinical Trials
- PMID: 33909022
- PMCID: PMC8082432
- DOI: 10.1001/jamacardio.2021.0852
Assessment of Catheter Ablation or Antiarrhythmic Drugs for First-line Therapy of Atrial Fibrillation: A Meta-analysis of Randomized Clinical Trials
Abstract
Importance: Early rhythm control of atrial fibrillation (AF) with either antiarrhythmic drugs (AADs) or catheter ablation has been reported to improve cardiovascular outcomes compared with usual care; however, the optimal therapeutic modality to achieve early rhythm control is unclear.
Objective: To assess the safety and efficacy of AF ablation as first-line therapy when compared with AADs in patients with paroxysmal AF.
Data sources: PubMed/MEDLINE, Scopus, Google Scholar, and various major scientific conference sessions from January 1, 2000, through November 23, 2020.
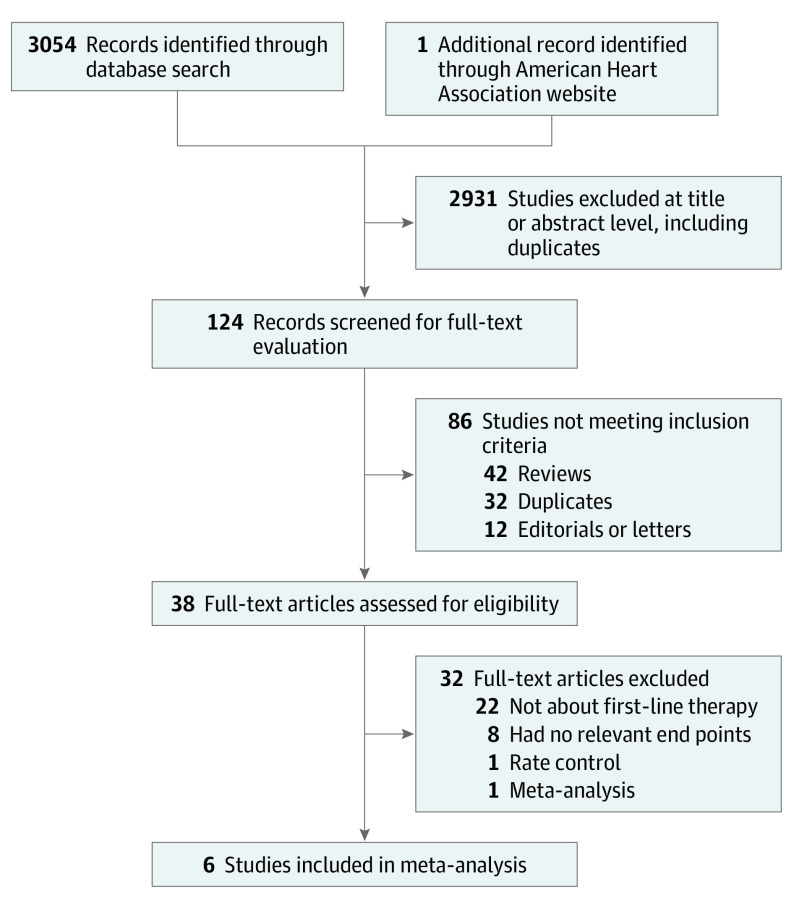
Study selection: Randomized clinical trials (RCTs) published in English that had at least 12 months of follow-up and compared clinical outcomes of ablation vs AADs as first-line therapy in adults with AF. The quality of individual studies was assessed using the Cochrane risk of bias tool. Six RCTs met inclusion criteria, including 1212 patients.
Data extraction and synthesis: Two investigators independently extracted data. Reporting was performed in compliance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines. Analysis was performed using a random-effects model with the Mantel-Haenszel method, and results are presented as 95% CIs.
Main outcomes and measures: Main outcomes were safety and efficacy of AF ablation as first-line therapy when compared with AADs. Trials were evaluated as having low risk of selection and attrition biases, high risk of performance bias, and with unclear risk for detection biases due to unblinding and open-label designs.
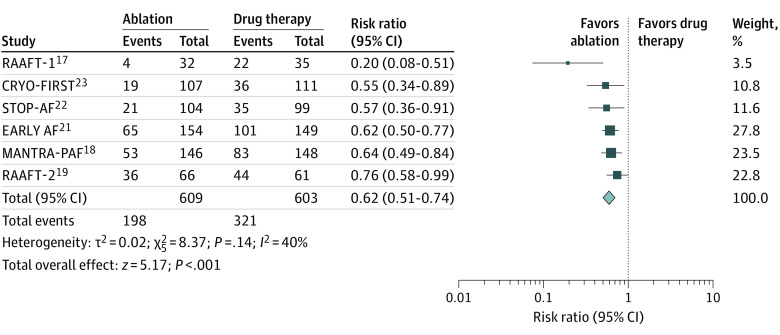
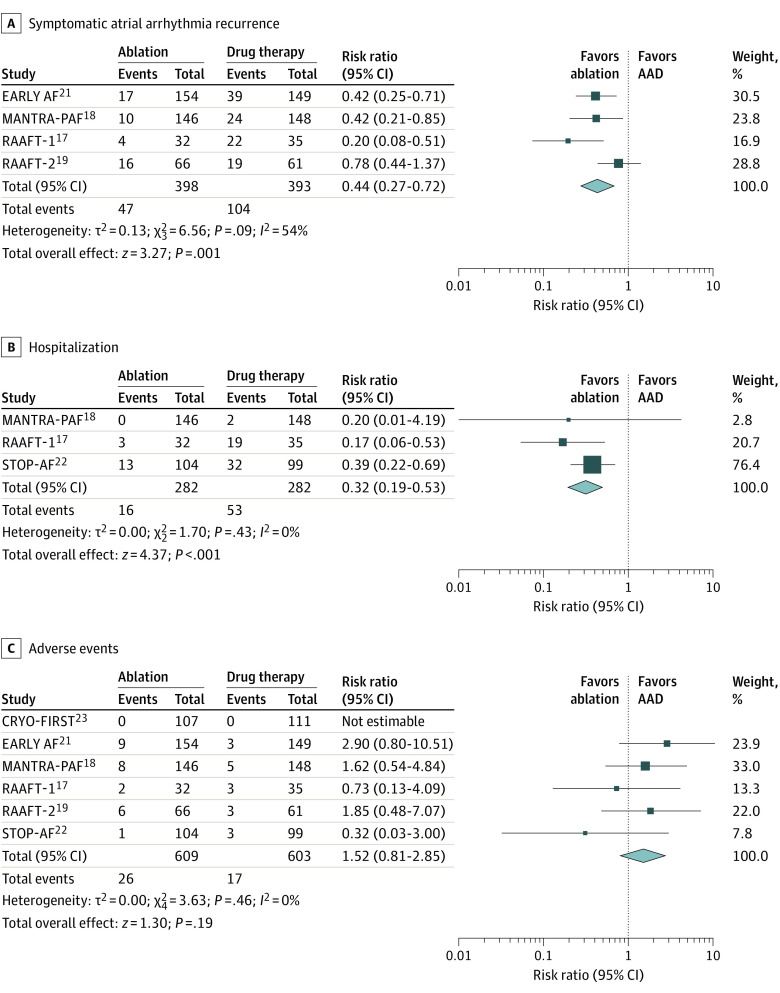
Results: A total of 6 RCTs involving 1212 patients with AF were included (609 were randomized to AF ablation and 603 to drug therapy; mean [SD] age, 56 [11] years). Compared with AADs, catheter ablation use was associated with reductions in recurrent atrial arrhythmia (32.3% vs 53%; risk ratio [RR], 0.62; 95% CI, 0.51-0.74; P < .001; I2 = 40%), with a number needed to treat with ablation to prevent 1 arrhythmia of 5. Use of ablation was also associated with reduced symptomatic atrial arrhythmia (11.8% vs 26.4%; RR, 0.44; 95% CI, 0.27-0.72; P = .001; I2 = 54%) and hospitalization (5.6% vs 18.7%; RR, 0.32; 95% CI, 0.19-0.53; P < .001) with no significant difference in serious adverse events between the groups (4.2% vs 2.8%; RR, 1.52; 95% CI, 0.81-2.85; P = .19).
Conclusions and relevance: In this meta-analysis of randomized clinical trials including first-line therapy of patients with paroxysmal AF, catheter ablation compared with antiarrhythmic drugs was associated with reductions in recurrence of atrial arrhythmias and hospitalizations, with no difference in major adverse events.
Conflict of interest statement
Figures
References
-
- Van Gelder IC, Hagens VE, Bosker HA, et al. ; Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation Study Group . A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med. 2002;347(23):1834-1840. doi: 10.1056/NEJMoa021375 - DOI - PubMed
-
- Carlsson J, Miketic S, Windeler J, et al. ; STAF Investigators . Randomized trial of rate-control versus rhythm-control in persistent atrial fibrillation: the Strategies of Treatment of Atrial Fibrillation (STAF) study. J Am Coll Cardiol. 2003;41(10):1690-1696. doi: 10.1016/S0735-1097(03)00332-2 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
