

Labor epidural analgesia versus without labor epidural analgesia for multiparous women: a retrospective case control study
- PMID: 33910504
- PMCID: PMC8080314
- DOI: 10.1186/s12871-021-01355-0
Labor epidural analgesia versus without labor epidural analgesia for multiparous women: a retrospective case control study
Abstract
Background: Labor epidural analgesia (LEA) effectively relieves the labor pain, but it is still not available consistently for multiparous women in many institutions because of their obviously shortened labor length.
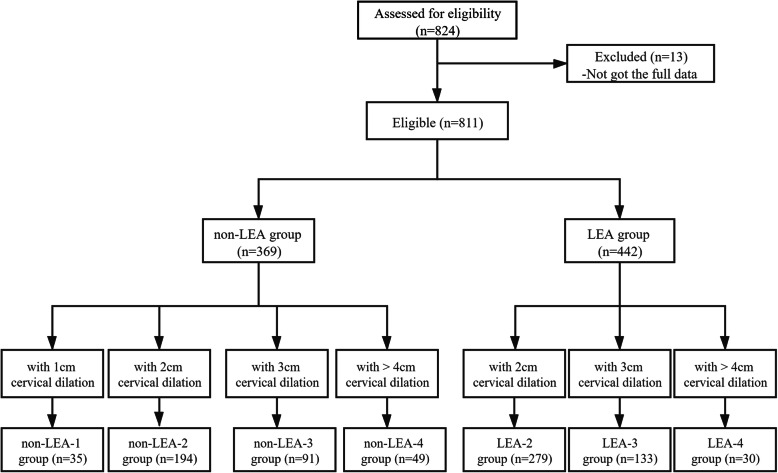
Methods: A total of 811 multiprous women were retrospective enrolled and firstly divided into two groups: LEA group or non-LEA group. And then they were divided into seven subgroups and analyzed according to the use of LEA and cervical dilation. The primary outcomes (time intervals, blood loss and Apgar scores) and secondary outcomes (maternal demographic characteristics and birth weight) were collected by checking electronic medical records.
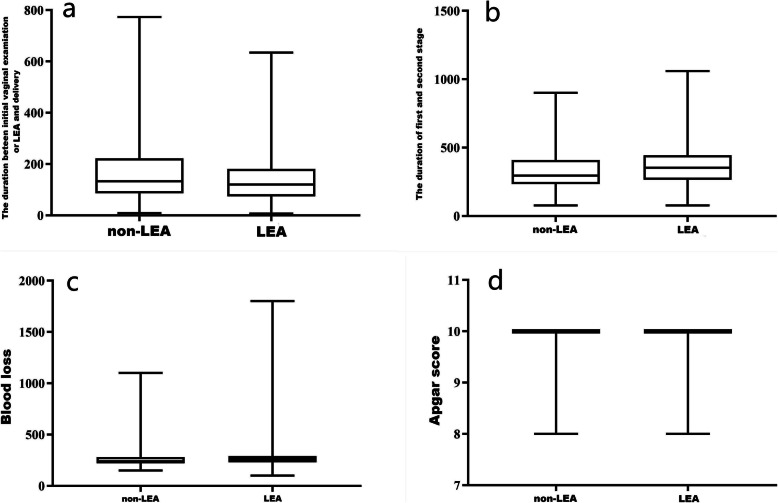
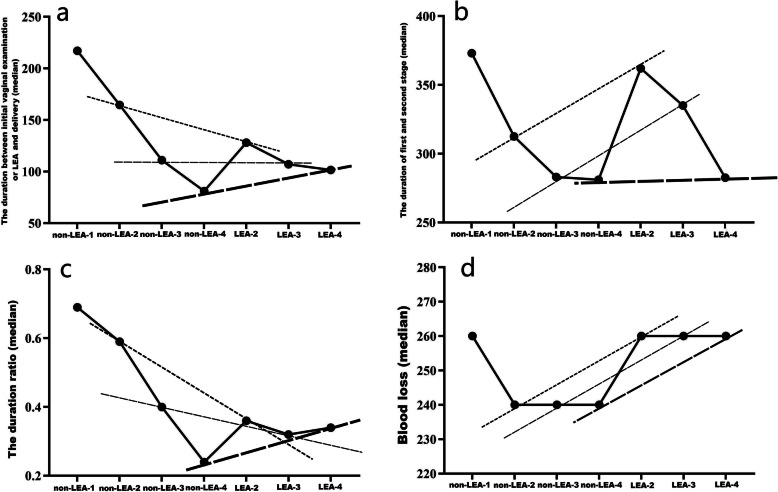
Results: The prevalence of using LEA in multiprous women was 54.5 %. Using LEA significantly lengthened the duration of labor stage by 56 min (P < 0.001), increased the blood loss (P < 0.001) and lowered Apgar scores (P = 0.001). In the comparison of sub-group analysis, using LEA can obviously prolong the duration of first-second stage in women with 2 cm cervical dilation (P < 0.001) and 3 cm cervical dilation (P = 0.014), while there was no significant difference with 4 cm or more cervical dilation (P = 0.69). Using LEA can significantly increased the blood loss when the initiation of LEA in the women with 2 cm cervical dilation (P < 0.001) and 3 cm cervical dilation (P = 0.035), meanwhile there were no significantly differences in the women with 4 cm or more cervical dilation (P = 0.524). Using LEA can significantly lower the Apgar scores when the initiation of LEA in the women with 2 cm cervical dilation (P = 0.001) and 4 cm or more cervical dilation (P = 0.025), while there were no significantly differences in the women with 3 cm cervical dilation (P = 0.839).
Conclusions: Labor epidural analgesia for the multiparous woman may alter progress of labor, increase postpartum blood loss and lower Apgar scores. Early or late initiation of LEA should be defined as with cervical dilatation of less or more than 3 cm and the different effect should be understand.
Trial registration: ChiCTR2100042746. Registered 27 January 2021-Prospectively registered, http://www.chictr.org.cn .
Keywords: Analgesia; Epidural; Labor duration; Labor stage; Maternal and neonatal outcomes; Multipara.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effects of epidural analgesia at 1 cm cervical dilatation on labor interventions in full-term primigravida: A retrospective cohort study.J Obstet Gynaecol Res. 2023 Jun;49(6):1545-1550. doi: 10.1111/jog.15640. Epub 2023 Mar 27. J Obstet Gynaecol Res. 2023. PMID: 36974387
-
Effects of early- and late- neuraxial analgesia on multiparous women: a retrospective monocentric study.BMC Anesthesiol. 2024 Jan 2;24(1):8. doi: 10.1186/s12871-023-02395-4. BMC Anesthesiol. 2024. PMID: 38166749 Free PMC article.
-
Effects of Patient-Controlled Epidural Analgesia on Uterine Electromyography During Spontaneous Onset of Labor in Term Nulliparous Women.Reprod Sci. 2015 Nov;22(11):1350-7. doi: 10.1177/1933719115578926. Epub 2015 Mar 29. Reprod Sci. 2015. PMID: 25824008
-
What is the slowest-yet-normal cervical dilation rate among nulliparous women with spontaneous labor onset?J Obstet Gynecol Neonatal Nurs. 2010 Jul-Aug;39(4):361-9. doi: 10.1111/j.1552-6909.2010.01154.x. J Obstet Gynecol Neonatal Nurs. 2010. PMID: 20629924 Free PMC article. Review.
-
Management of Spontaneous Vaginal Delivery.Am Fam Physician. 2024 Jun;109(6):525-532. Am Fam Physician. 2024. PMID: 38905550 Review.
Cited by
-
Impact of Intraspinal Nerve Block Anesthesia on Intrapartum Fever and the Neonate.Evid Based Complement Alternat Med. 2022 May 29;2022:2600755. doi: 10.1155/2022/2600755. eCollection 2022. Evid Based Complement Alternat Med. 2022. Retraction in: Evid Based Complement Alternat Med. 2023 Jun 21;2023:9862717. doi: 10.1155/2023/9862717. PMID: 35677370 Free PMC article. Retracted.
-
Effects of Early and Late Labor Epidural Analgesia on Multiparous Women: A Retrospective Monocentric Study.Cureus. 2025 May 26;17(5):e84825. doi: 10.7759/cureus.84825. eCollection 2025 May. Cureus. 2025. PMID: 40568290 Free PMC article.
-
Association between Parity and Preterm Birth-Retrospective Analysis from a Single Center in Poland.Healthcare (Basel). 2023 Jun 15;11(12):1763. doi: 10.3390/healthcare11121763. Healthcare (Basel). 2023. PMID: 37372882 Free PMC article.
-
Intrathecal Injection of Ropivacaine Reduces Cervical Resistance in Late-Pregnant Rats.Drug Des Devel Ther. 2022 Apr 26;16:1183-1189. doi: 10.2147/DDDT.S352411. eCollection 2022. Drug Des Devel Ther. 2022. PMID: 35502424 Free PMC article.
References
-
- Høtoft D, Maimburg RD. Epidural analgesia during birth and adverse neonatal outcomes: A population-based cohort study [published online ahead of print, 2020 Jun 18] Women Birth. 2020;S1871-5192(20):30265–1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
