

Developing and validating a risk algorithm to diagnose Neisseria gonorrhoeae and Chlamydia trachomatis in symptomatic Rwandan women
- PMID: 33910514
- PMCID: PMC8080377
- DOI: 10.1186/s12879-021-06073-z
Developing and validating a risk algorithm to diagnose Neisseria gonorrhoeae and Chlamydia trachomatis in symptomatic Rwandan women
Abstract
Background: Algorithms that bridge the gap between syndromic sexually transmitted infection (STI) management and treatment based in realistic diagnostic options and local epidemiology are urgently needed across Africa. Our objective was to develop and validate a risk algorithm for Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT) diagnosis among symptomatic Rwandan women and to compare risk algorithm performance to the current Rwandan National Criteria for NG/CT diagnosis.
Methods: The risk algorithm was derived in a cohort (n = 468) comprised of symptomatic women in Kigali who sought free screening and treatment for sexually transmitted infections and vaginal dysbioses at our research site. We used logistic regression to derive a risk algorithm for prediction of NG/CT infection. Ten-fold cross-validation internally validated the risk algorithm. We applied the risk algorithm to an external validation cohort also comprised of symptomatic Rwandan women (n = 305). Measures of calibration, discrimination, and screening performance of our risk algorithm compared to the current Rwandan National Criteria are presented.
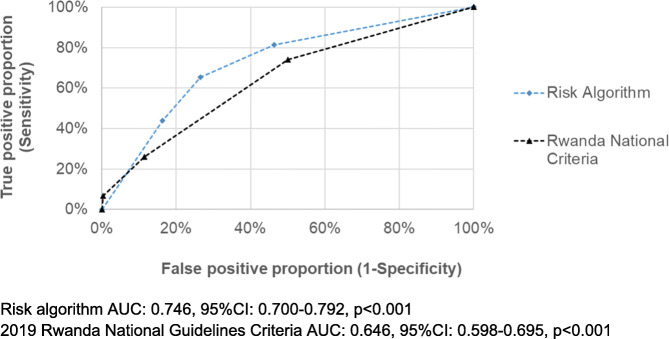
Results: The prevalence of NG/CT in the derivation cohort was 34.6%. The risk algorithm included: age < =25, having no/primary education, not having full-time employment, using condoms only sometimes, not reporting genital itching, testing negative for vaginal candida, and testing positive for bacterial vaginosis. The model was well calibrated (Hosmer-Lemeshow p = 0.831). Higher risk scores were significantly associated with increased prevalence of NG/CT infection (p < 0.001). Using a cut-point score of > = 5, the risk algorithm had a sensitivity of 81%, specificity of 54%, positive predictive value (PPV) of 48%, and negative predictive value (NPV) of 85%. Internal and external validation showed similar predictive ability of the risk algorithm, which outperformed the Rwandan National Criteria. Applying the Rwandan National Criteria cutoff of > = 2 (the current cutoff) to our derivation cohort had a sensitivity of 26%, specificity of 89%, PPV of 55%, and NPV of 69%.
Conclusions: These data support use of a locally relevant, evidence-based risk algorithm to significantly reduce the number of untreated NG/CT cases in symptomatic Rwandan women. The risk algorithm could be a cost-effective way to target treatment to those at highest NG/CT risk. The algorithm could also aid in sexually transmitted infection risk and prevention communication between providers and clients.
Keywords: Chlamydia trachomatis; Neisseria gonorrhoeae; Risk algorithm; Rwanda.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Etiologies of genital inflammation and ulceration in symptomatic Rwandan men and women responding to radio promotions of free screening and treatment services.PLoS One. 2021 Apr 20;16(4):e0250044. doi: 10.1371/journal.pone.0250044. eCollection 2021. PLoS One. 2021. PMID: 33878134 Free PMC article.
-
Performance of syndromic management for the detection and treatment of genital Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis among women attending antenatal, well woman and sexual health clinics in Papua New Guinea: a cross-sectional study.BMJ Open. 2017 Dec 29;7(12):e018630. doi: 10.1136/bmjopen-2017-018630. BMJ Open. 2017. PMID: 29288183 Free PMC article.
-
Chlamydia trachomatis, Neisseria gonorrhoea, and Trichomonas vaginalis infections among pregnant women and male partners in Dutch midwifery practices: prevalence, risk factors, and perinatal outcomes.Reprod Health. 2021 Jun 26;18(1):132. doi: 10.1186/s12978-021-01179-8. Reprod Health. 2021. PMID: 34174905 Free PMC article.
-
Genital Chlamydia trachomatis and Neisseria gonorrhoeae infections among women in sub-Saharan Africa: A structured review.Int J STD AIDS. 2018 Jul;29(8):806-824. doi: 10.1177/0956462418758224. Epub 2018 Feb 28. Int J STD AIDS. 2018. PMID: 29486628 Review.
-
[Prevalence of anti-Chlamydia trachomatis and anti-Neisseria gonorrhoeae antibodies in Mexican populations].Salud Publica Mex. 2003;45 Supp 5:S681-9. Salud Publica Mex. 2003. PMID: 14974280 Review. Spanish.
Cited by
-
Derivation and Internal Validation of a Risk Score for Predicting Chlamydia trachomatis Infection in Kenyan Women Planning Conception.Sex Transm Dis. 2023 Sep 1;50(9):625-633. doi: 10.1097/OLQ.0000000000001795. Epub 2023 Jul 3. Sex Transm Dis. 2023. PMID: 36877639 Free PMC article.
-
Identifying youth at high risk for sexually transmitted infections in community-based settings using a risk prediction tool: a validation study.BMC Infect Dis. 2021 Dec 8;21(1):1234. doi: 10.1186/s12879-021-06937-4. BMC Infect Dis. 2021. PMID: 34879820 Free PMC article. Clinical Trial.
References
-
- Rowley J, Vander Hoorn S, Korenromp E, Low N, Unemo M, Abu-Raddad LJ, Chico RM, Smolak A, Newman L, Gottlieb S, Thwin SS, Broutet N, Taylor MM. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. 2019;97(8):548–62P. doi: 10.2471/BLT.18.228486. - DOI - PMC - PubMed
-
- Takuva S, Mugurungi O, Mutsvangwa J, Machiha A, Mupambo AC, Maseko V, Cham F, Mungofa S, Mason P, Lewis DA. Etiology and antimicrobial susceptibility of pathogens responsible for urethral discharge among men in Harare. Zimbabwe Sex Transm Dis. 2014;41(12):713–717. doi: 10.1097/OLQ.0000000000000204. - DOI - PubMed
-
- Chirenje ZM, Dhibi N, Handsfield HH, Gonese E, Tippett Barr B, Gwanzura L, Latif AS, Maseko DV, Kularatne RS, Tshimanga M, Kilmarx PH, Machiha A, Mugurungi O, Rietmeijer CA. The Etiology of Vaginal Discharge Syndrome in Zimbabwe: Results from the Zimbabwe STI Etiology Study. Sex Transm Dis. 2018;45(6):422–428. doi: 10.1097/OLQ.0000000000000771. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
