

Major complications of dural venous sinus stenting for idiopathic intracranial hypertension: case series and management considerations
- PMID: 33911014
- PMCID: PMC8722449
- DOI: 10.1136/neurintsurg-2021-017361
Major complications of dural venous sinus stenting for idiopathic intracranial hypertension: case series and management considerations
Abstract
Background: Venous sinus stenting (VSS) is a safe, effective, and increasingly popular treatment option for selected patients with idiopathic intracranial hypertension (IIH). Serious complications associated with VSS are rarely reported.
Methods: Serious complications after VSS were identified retrospectively from multicenter databases. The cases are presented and management strategies are discussed.
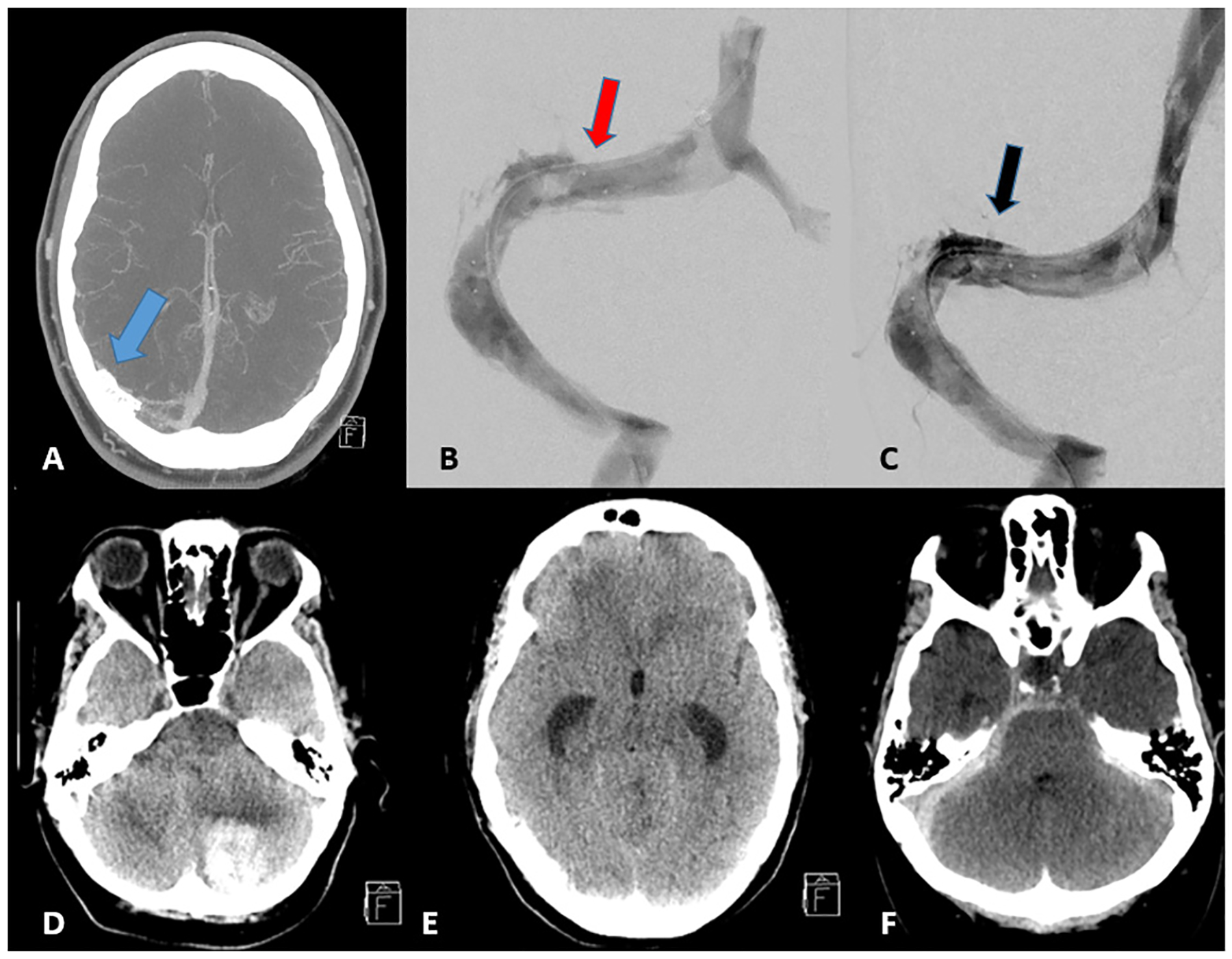
Results: Six major acute and chronic complications after VSS were selected from a total of 811 VSS procedures and 1466 venograms for IIH. These included an acute subdural hematoma from venous extravasation, cases of both intraprocedural and delayed stent thrombosis, an ultimately fatal cerebellar hemorrhage resulting in acute obstructive hydrocephalus, venous microcatheter perforation during venography and manometry, and a patient who developed subarachnoid hemorrhage and subdural hematoma after cerebellar cortical vein perforation. The six cases are reviewed and learning points regarding complication avoidance and management are presented.
Conclusion: We report on six rare, major complications after VSS for IIH. Familiarity with these potential complications and appropriate timely management may allow for good clinical outcomes.
Keywords: complication; stent; vein.
© Author(s) (or their employer(s)) 2022. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KMF- Associate Editor, Journal of Neurointerventional Surgery.
Figures



References
-
- Markey KA, Mollan SP, Jensen RH, et al. Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol 2016;15:78–91. - PubMed
-
- Giridharan N, Patel SK, Ojugbeli A, et al. Understanding the complex pathophysiology of idiopathic intracranial hypertension and the evolving role of venous sinus stenting: a comprehensive review of the literature. Neurosurg Focus 2018;45:E10. - PubMed
-
- Leishangthem L, SirDeshpande P, Dua D, et al. Dural venous sinus stenting for idiopathic intracranial hypertension: an updated review. J Neuroradiol 2019;46:148–54. - PubMed
-
- Nicholson P, Brinjikji W, Radovanovic I, et al. Venous sinus stenting for idiopathic intracranial hypertension: a systematic review and meta-analysis. J Neurointerv Surg 2019;11:380–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources