

Post Kala-Azar Dermal Leishmaniasis: Clinical Features and Differential Diagnosis
- PMID: 33911290
- PMCID: PMC8061484
- DOI: 10.4103/ijd.IJD_602_20
Post Kala-Azar Dermal Leishmaniasis: Clinical Features and Differential Diagnosis
Abstract
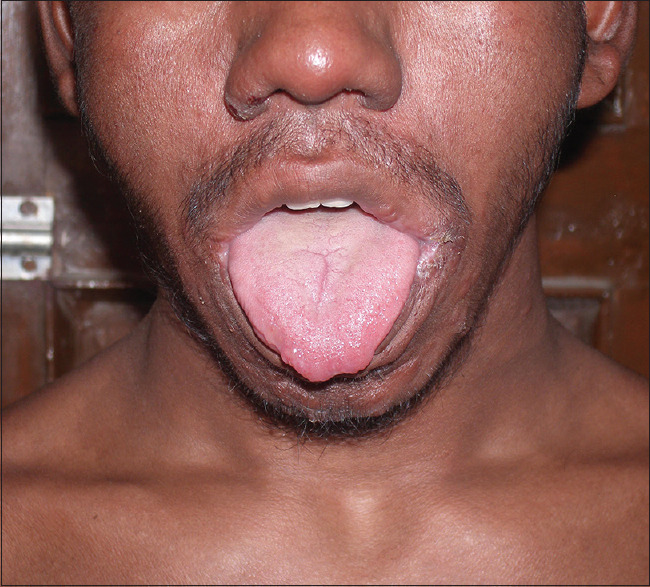
Post kala-azar dermal leishmaniasis (PKDL) is a mucocutaneous disease usually seen in apparently cured, inadequately treated or untreated cases of visceral leishmaniasis and is endemic to many parts of India, Nepal, Bangladesh, and eastern Africa (Sudan, Ethiopia, Kenya). The disease usually manifests as a variable combination of hypopigmented patches, erythematous succulent papulo-plaques, and nodular lesions on the face and upper body and sometimes extending on the extremities, genitalia, and tongue. Atypical morphology and presentations are not uncommon, especially in endemic areas, which include photosensitivity, verrucous, hypertrophic, xanthomatous, and ulcerative lesions. Recognition of spectrum of mucocutaneous changes helps physicians in early initiation of treatment and in reducing disease transmission in the community. The differential diagnosis depends on the pattern of manifestations, but lepromatous leprosy is the closest mimicker. Since PKDL does not cause significant morbidity, at least initially, but the affected patients continue to act as a reservoir of the disease, active case detection is required to identify cases early to control the disease transmission in the community.
Keywords: Active surveillance; India; Leishmania donovani; Sudan; para kala-azar dermal leishmaniasis; post kala-azar dermal leishmaniasis; visceral leishmaniasis.
Copyright: © 2021 Indian Journal of Dermatology.
Conflict of interest statement
There are no conflicts of interest.
Figures

























References
LinkOut - more resources
Full Text Sources
Other Literature Sources