

Accuracy of OMI ECG findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction
- PMID: 33912650
- PMCID: PMC8065286
- DOI: 10.1016/j.ijcha.2021.100767
Accuracy of OMI ECG findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction
Abstract
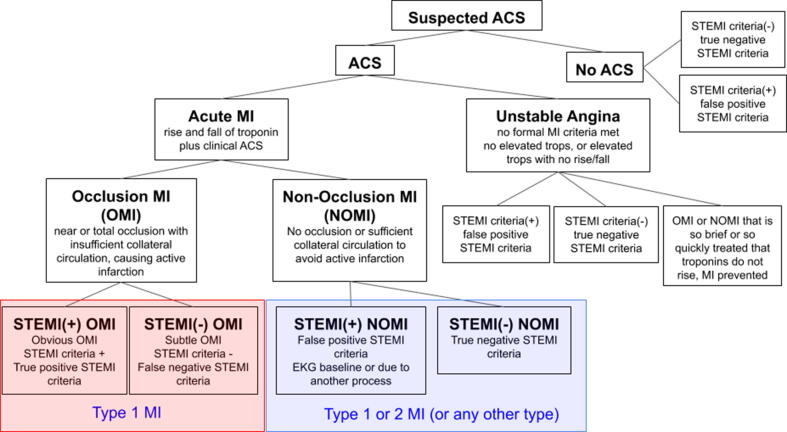
Objective: In the STEMI paradigm of Acute Myocardial Infarction (AMI), many NSTEMI patients have unrecognized acute coronary occlusion MI (OMI), may not receive emergent reperfusion, and have higher mortality than NSTEMI patients without occlusion. We have proposed a new OMI vs. Non-Occlusion MI (NOMI) paradigm shift. We sought to compare the diagnostic accuracy of OMI ECG findings vs. formal STEMI criteria for the diagnosis of OMI. We hypothesized that blinded interpretation for predefined OMI ECG findings would be more accurate than STEMI criteria for the diagnosis of OMI.
Methods: We performed a retrospective case-control study of patients with suspected acute coronary syndrome. The primary definition of OMI was either 1) acute TIMI 0-2 flow culprit or 2) TIMI 3 flow culprit with peak troponin T 1.0 ng/mL or I 10.0 ng/mL.
Results: 808 patients were included, of whom 49% had AMI (33% OMI; 16% NOMI). Sensitivity, specificity, and accuracy of STEMI criteria vs Interpreter 1 using OMI ECG findings among 808 patients were 41% vs 86%, 94% vs 91%, and 77% vs 89%, and for Interpreter 2 among 250 patients were 36% vs 80%, 91% vs 92%, and 76% vs 89%. STEMI(-) OMI patients had similar infarct size and mortality as STEMI(+) OMI patients, but greater delays to angiography.
Conclusions: Blinded interpretation using predefined OMI ECG findings was superior to STEMI criteria for the ECG diagnosis of Occlusion MI. These data support further investigation into the OMI vs. NOMI paradigm and suggest that STEMI(-) OMI patients could be identified rapidly and noninvasively for emergent reperfusion using more accurate ECG interpretation.
Keywords: ACS, Acute coronary syndrome; AMI, acute myocardial infarction; Acute coronary syndromes; ECG, Electrocardiogram; ED, Emergency department; Electrocardiography; LBBB, Left Bundle Branch Block; MIRO, Myocardial Infarction Ruled Out; MSC, Modified Sgarbossa Criteria; NOMI, Non-occlusion myocardial infarction; NSTEMI, Non-ST-segment elevation myocardial infarction; OMI, Occlusion myocardial infarction; Occlusion myocardial infarction; ST elevation myocardial infarction; STD, ST-segment depression; STE, ST-segment elevation; STEMI, ST-segment elevation myocardial infarction; VPR, Ventricular Paced Rhythm.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group, Lancet 343 (1994) 311–322. - PubMed
-
- Khan A.R. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur. Heart J. 2017;38:3082–3089. - PubMed
-
- McCabe J.M. Prevalence and factors associated with false-positive ST-segment elevation myocardial infarction diagnoses at primary percutaneous coronary intervention–capable centers: a report from the Activate-SF registry. Arch. Intern. Med. 2012;172:864–871. - PubMed
-
- Larson D.M. ‘False-positive’ cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. JAMA. 2007;298:2754–2760. - PubMed
-
- Kontos M.C. An evaluation of the accuracy of emergency physician activation of the cardiac catheterization laboratory for patients with suspected ST-segment elevation myocardial infarction. Ann. Emerg. Med. 2010;55:423–430. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
