

Rituximab in Membranous Nephropathy
- PMID: 33912740
- PMCID: PMC8071613
- DOI: 10.1016/j.ekir.2020.12.035
Rituximab in Membranous Nephropathy
Abstract
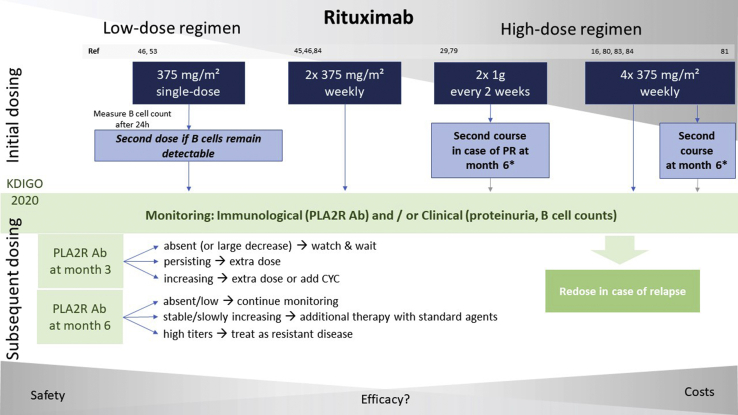
Membranous nephropathy (MN) is the most common cause of primary nephrotic syndrome among adults. The identification of phospholipase A2 receptor (PLA2R) as target antigen in most patients changed the management of MN dramatically, and provided a rationale for B-cell depleting agents such as rituximab. The efficacy of rituximab in inducing remission has been investigated in several studies, including 3 randomized controlled trials, in which complete and partial remission of proteinuria was achieved in approximately two-thirds of treated patients. Due to its favorable safety profile, rituximab is now considered a first-line treatment option for MN, especially in patients at moderate and high risk of deterioration in kidney function. However, questions remain about how to best use rituximab, including the optimal dosing regimen, a potential need for maintenance therapy, and assessment of long-term safety and efficacy outcomes. In this review, we provide an overview of the current literature and discuss both strengths and limitations of "the new standard."
Keywords: B cells; membranous nephropathy; nephrotic syndrome; rituximab.
© 2021 Published by Elsevier, Inc., on behalf of the International Society of Nephrology.
Figures
Comment in
-
Bortezomib plus dexamethasone for rituximab-resistant PLA2R+ membranous nephropathy.Kidney Int. 2021 Sep;100(3):708-709. doi: 10.1016/j.kint.2021.04.011. Kidney Int. 2021. PMID: 34420663 No abstract available.
References
-
- Barbour S.J., Greenwald A., Djurdjev O. Disease-specific risk of venous thromboembolic events is increased in idiopathic glomerulonephritis. Kidney Int. 2012;81:190–195. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
