

The Role of Glomerular Epithelial Injury in Kidney Function Decline in Patients With Diabetic Kidney Disease in the TRIDENT Cohort
- PMID: 33912757
- PMCID: PMC8071659
- DOI: 10.1016/j.ekir.2021.01.025
The Role of Glomerular Epithelial Injury in Kidney Function Decline in Patients With Diabetic Kidney Disease in the TRIDENT Cohort
Abstract
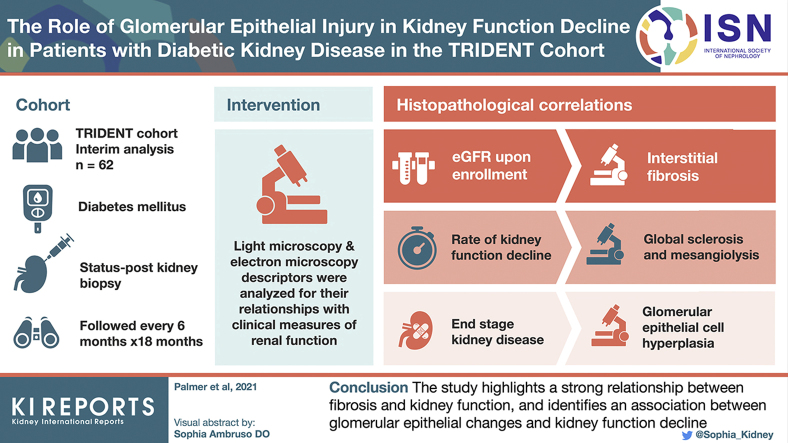
Introduction: Although diabetic kidney disease (DKD) is responsible for more than half of all chronic and end-stage kidney disease (ESKD), the association of light (LM) and electron microscopic (EM) structural changes with clinical parameters and prognosis in DKD is incompletely understood.
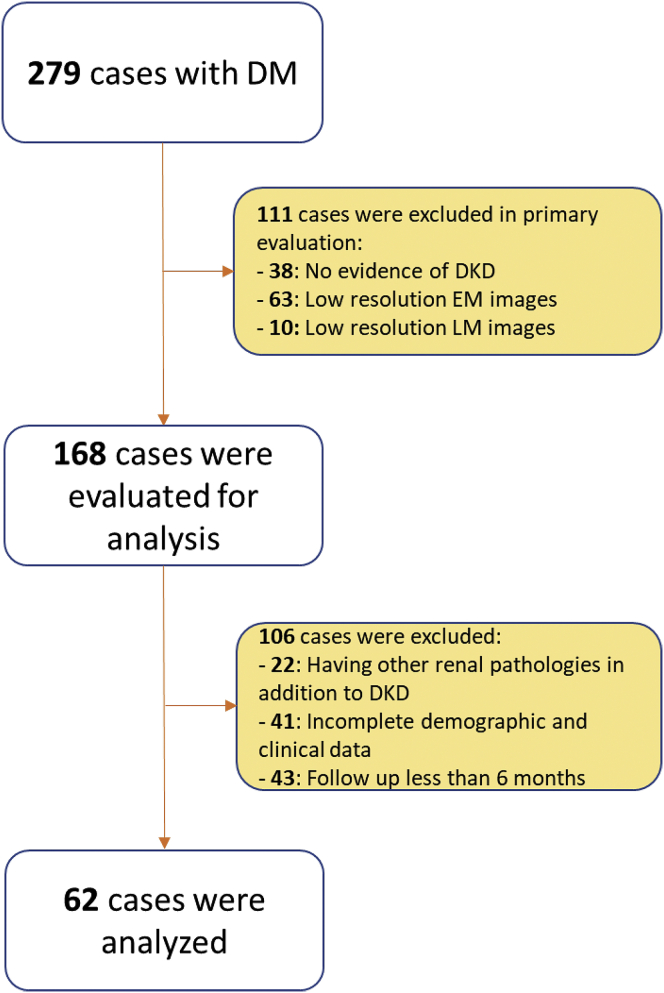
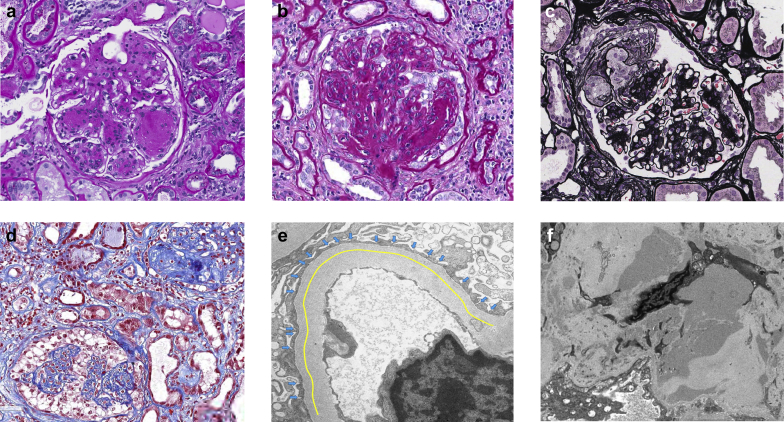
Methods: This is an interim analysis of 62 patients diagnosed with biopsy-confirmed DKD from the multicenter TRIDENT (Transformative Research in Diabetic Nephropathy) study. Twelve LM and 8 EM descriptors, representing changes in glomeruli, tubulointerstitium, and vasculature were analyzed for their relationship with clinical measures of renal function. Patients were followed every 6 months.
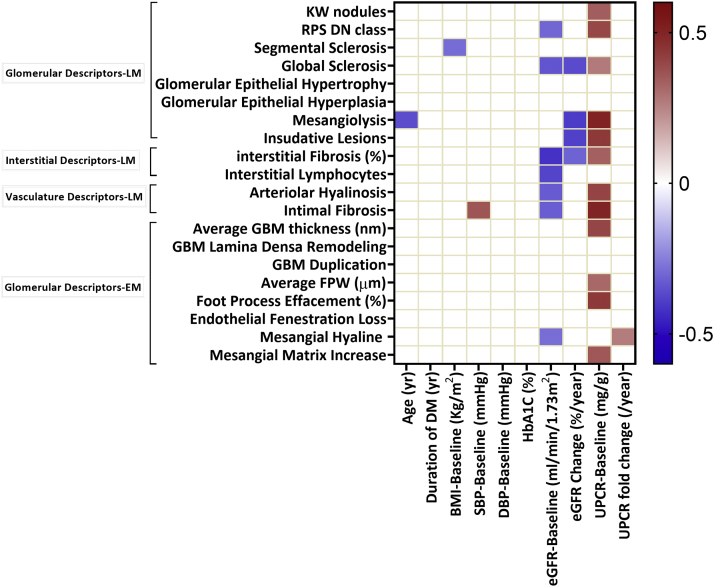
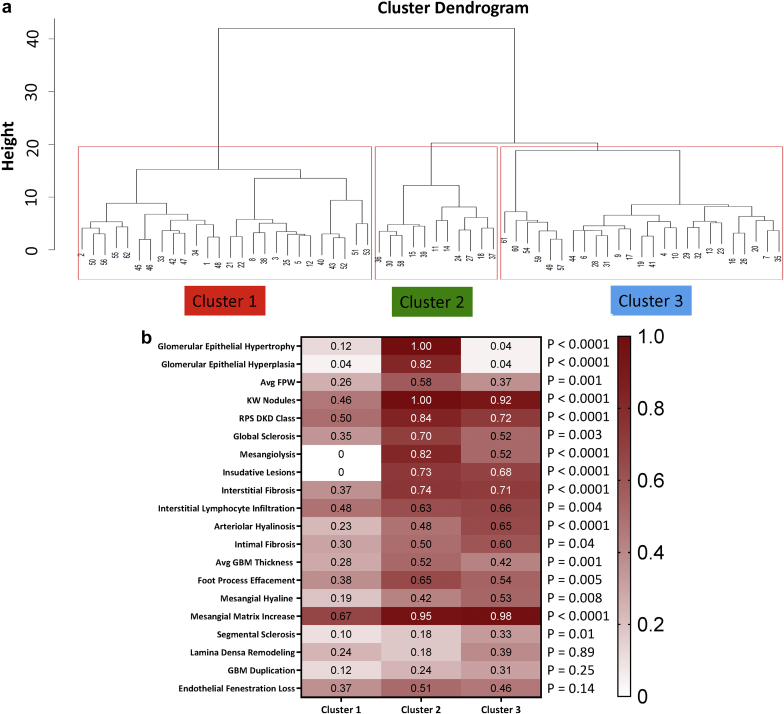
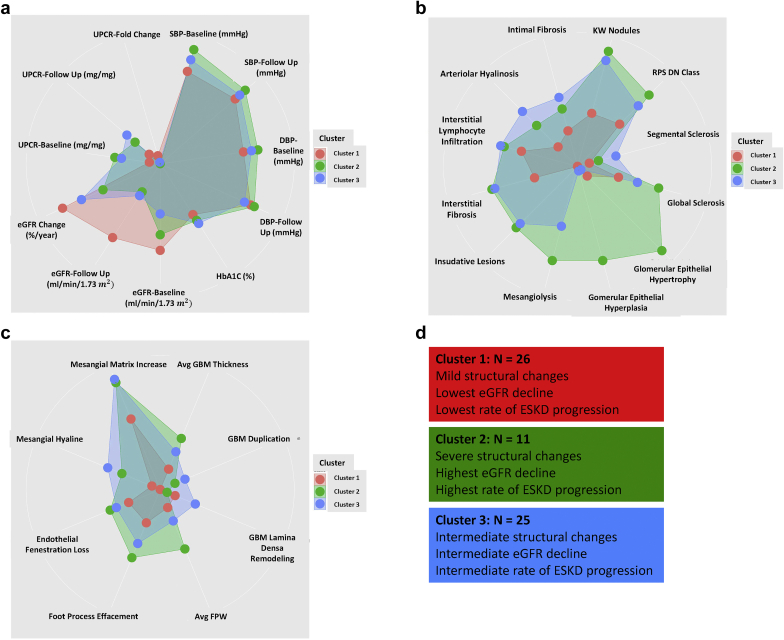
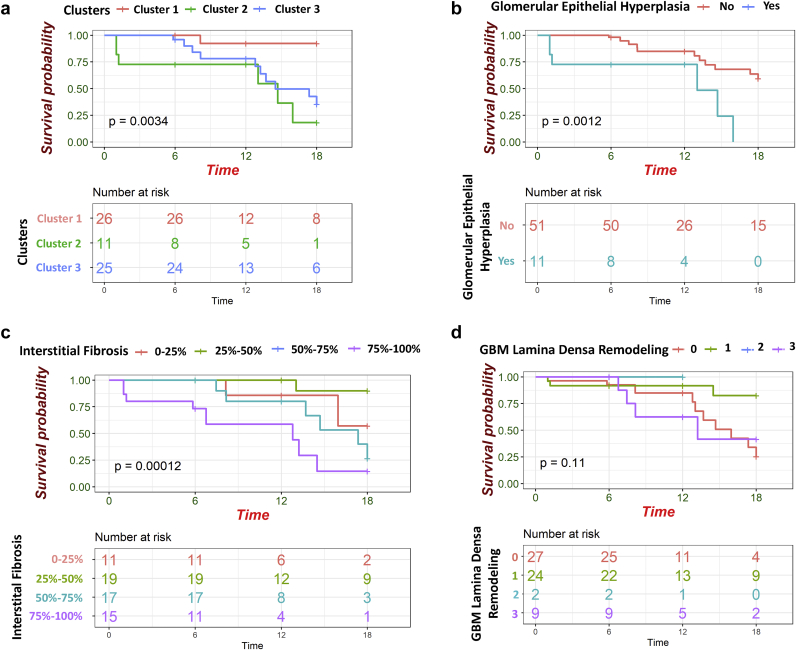
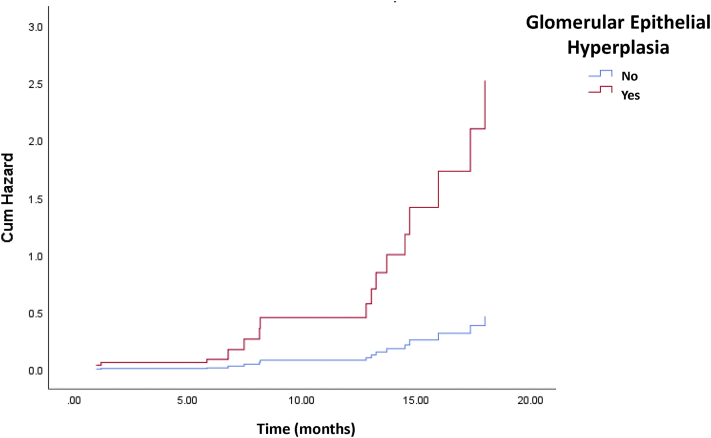
Results: Multivariable linear regression analysis revealed that estimated glomerular filtration rate (eGFR) upon enrollment correlated the best with interstitial fibrosis. On the other hand, the rate of kidney function decline (eGFR slope) correlated the most with glomerular lesions including global glomerulosclerosis and mesangiolysis. Unbiased clustering analysis based on histopathologic data identified 3 subgroups. The first cluster, encompassing subjects with the mildest histologic lesions, had the most preserved kidney function. The second and third clusters had similar degrees of kidney dysfunction and structural damage, but differed in the degree of glomerular epithelial cell and podocyte injury (podocytopathy DKD subtype). Cox proportional hazard analysis showed that subjects in cluster 2 had the highest risk to reach ESKD (hazard ratio: 17.89; 95% confidence interval: 2.13-149.79). Glomerular epithelial hyperplasia and interstitial fibrosis were significant predictors of ESKD in the multivariate model.
Conclusion: The study highlights the association between fibrosis and kidney function and identifies the role of glomerular epithelial changes and kidney function decline.
Keywords: diabetic kidney disease; end-stage kidney disease; glomerular epithelial injury; kidney function; pathological descriptors.
© 2021 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Wen C.P., Chang C.H., Tsai M.K. Diabetes with early kidney involvement may shorten life expectancy by 16 years. Kidney Int. 2017;92:388–396. - PubMed
-
- Ameh O.I., Okpechi I.G., Agyemang C. Global, regional, and ethnic differences in diabetic nephropathy. In: Roelofs J.J., Vogy L., editors. Diabetic Nephropathy. Springer; Cham, Switzerland: 2019. pp. 33–44.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
