

Human Immunodeficiency Virus Infection in Adolescents and Mode of Transmission in Southern Africa: A Multinational Analysis of Population-Based Survey Data
- PMID: 33912973
- PMCID: PMC8366830
- DOI: 10.1093/cid/ciab031
Human Immunodeficiency Virus Infection in Adolescents and Mode of Transmission in Southern Africa: A Multinational Analysis of Population-Based Survey Data
Abstract
Background: Adolescents aged 10-19 years living with human immunodeficiency virus (HIV) (ALHIV), both perinatally infected adolescents (APHIV) and behaviorally infected adolescents (ABHIV), are a growing population with distinct care needs. We characterized the epidemiology of HIV in adolescents included in Population-based HIV Impact Assessments (2015-2017) in Zimbabwe, Malawi, Zambia, Eswatini, and Lesotho.
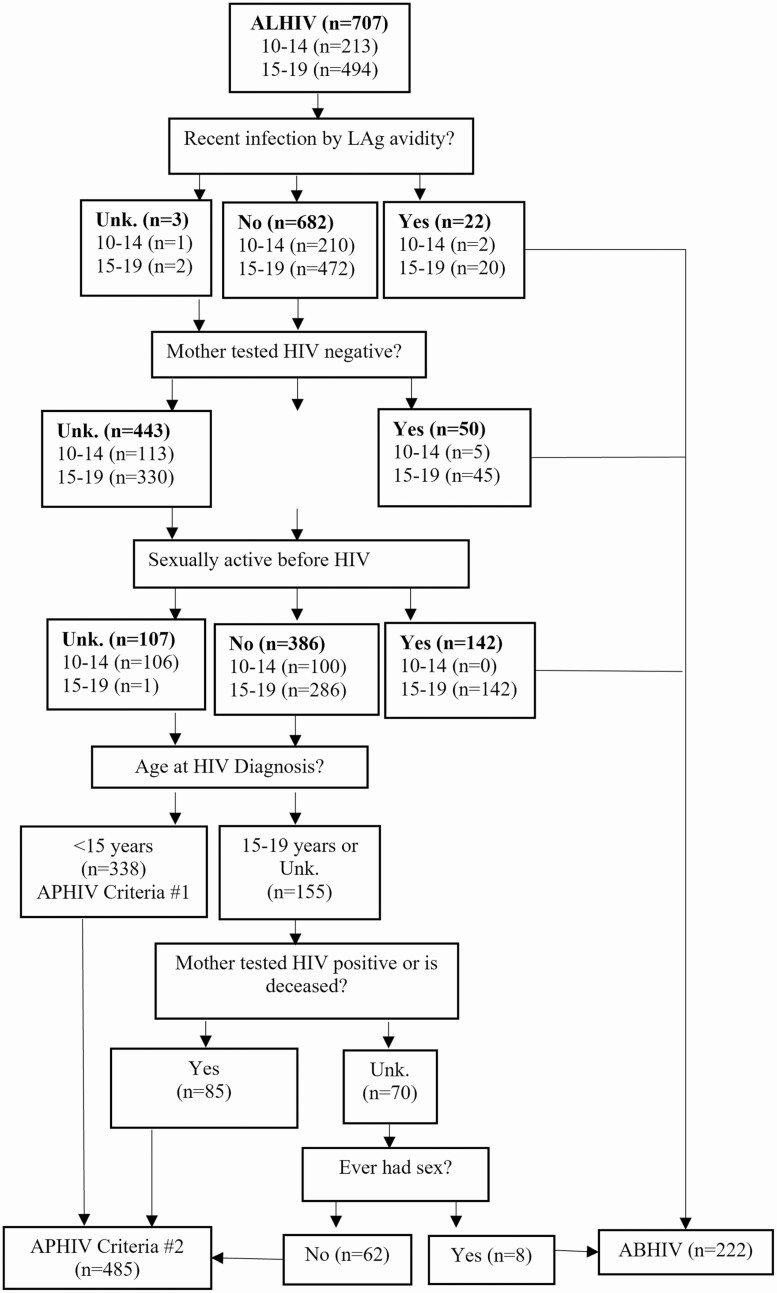
Methods: Adolescents were tested for HIV using national rapid testing algorithms. Viral load (VL) suppression (VLS) was defined as VL <1000 copies/mL, and undetectable VL (UVL) as VL <50 copies/mL. Recent infection (within 6 months) was measured using a limiting antigen avidity assay, excluding adolescents with VLS or with detectable antiretrovirals (ARVs) in blood. To determine the most likely mode of infection, we used a risk algorithm incorporating recency, maternal HIV and vital status, history of sexual activity, and age at diagnosis.
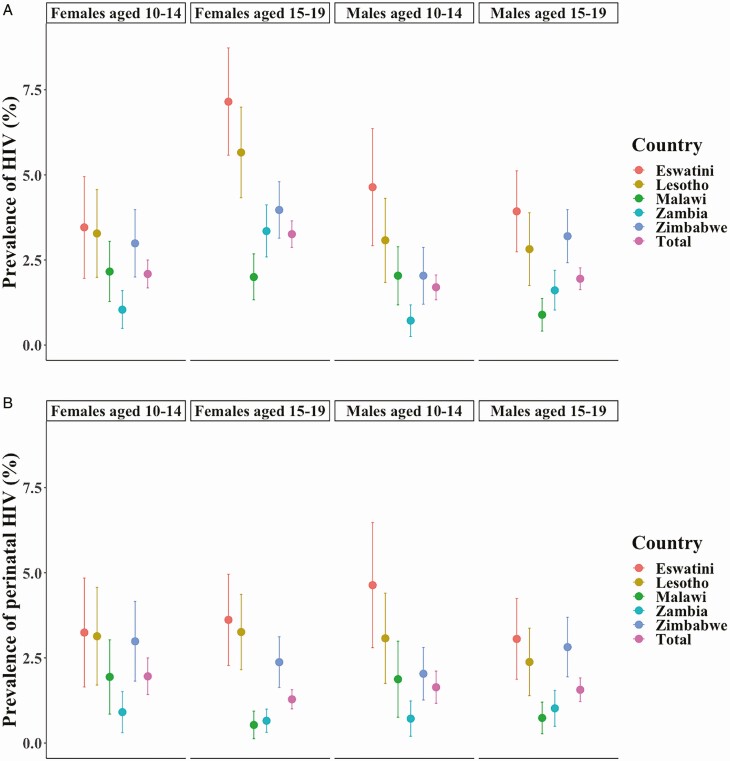
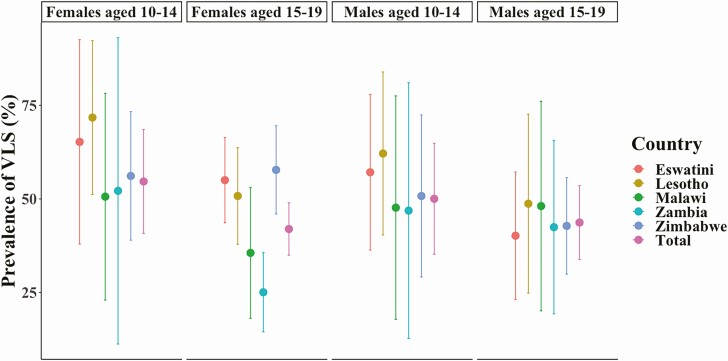
Results: HIV prevalence ranged from 1.6% in Zambia to 4.8% in Eswatini. Of 707 ALHIV, 60.9% (95% confidence interval, 55.3%-66.6%) had HIV previously diagnosed, and 47.1% (41.9%-52.3%) had VLS. Our algorithm estimated that 72.6% of ALHIV (485 of 707) were APHIV, with HIV diagnosed previously in 69.5% of APHIV and 39.4% of ABHIV, and with 65.3% of APHIV and 33.5% of ABHIV receiving ARV treatment. Only 67.2% of APHIV and 60.5% of ABHIV receiving ARVs had UVL.
Conclusions: These findings suggest that two-thirds of ALHIV were perinatally infected, with many unaware of their status. The low prevalence of VLS and UVL in those receiving treatment raises concerns around treatment effectiveness. Expansion of opportunities for HIV diagnoses and the optimization of treatment are imperative.
Keywords: HIV; adolescents; national survey data; perinatal HIV infection; southern Africa.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- UNICEF. HIV and AIDS in adolescents. Available at: https://data.unicef.org/topic/adolescents/hiv-aids/. Accessed 30 September 2019.
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F; Ghent International AIDS Society (IAS) Working Group on HIV Infection in Women and Children . Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet 2004; 364:1236–43. - PubMed
-
- Joint United Nations Programme on HIV/AIDS. Improving UNAIDS’ paediatric and adolescent estimates. Available at: http://www.unaids.org/sites/default/files/media_asset/improving-unaids-p.... Accessed 19 July 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
