

Compromised extraction sockets: a new classification and prevalence involving both soft and hard tissue loss
- PMID: 33913633
- PMCID: PMC8090797
- DOI: 10.5051/jpis.2005120256
Compromised extraction sockets: a new classification and prevalence involving both soft and hard tissue loss
Abstract
Purpose: Previous studies have solely focused on fresh extraction sockets, whereas in clinical settings, alveolar sockets are commonly associated with chronic inflammation. Because the extent of tissue destruction varies depending on the origin and the severity of inflammation, infected alveolar sockets may display various configurations of their remaining soft and hard tissues following tooth extraction. The aim of this study was to classify infected alveolar sockets and to provide the appropriate treatment approaches.
Methods: A proposed classification of extraction sockets with chronic inflammation was developed based upon the morphology of the bone defect and soft tissue at the time of tooth extraction. The prevalence of each type of the suggested classification was determined retrospectively in a cohort of patients who underwent, between 2011 and 2015, immediate bone grafting procedures (ridge preservation/augmentation) after tooth extractions at Seoul National University Dental Hospital.
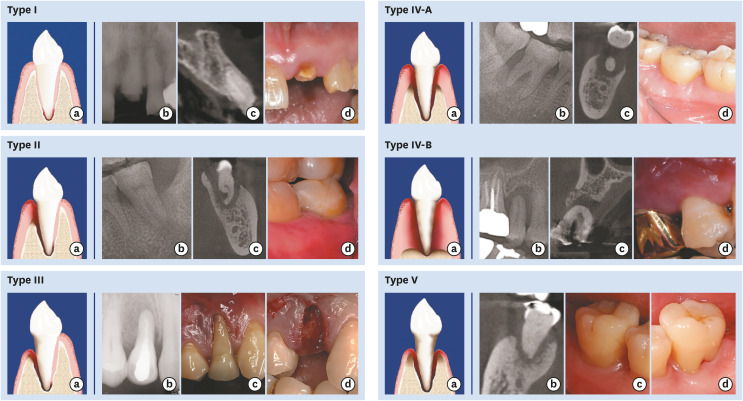
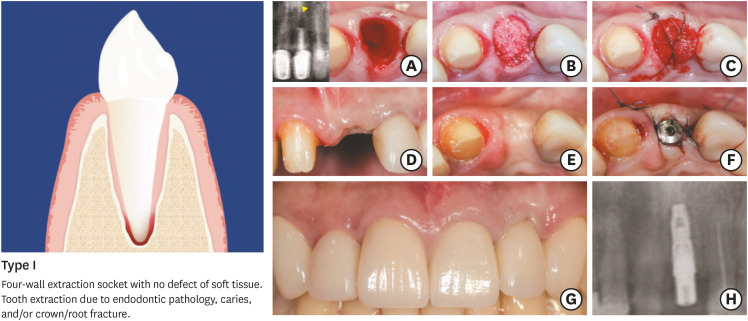
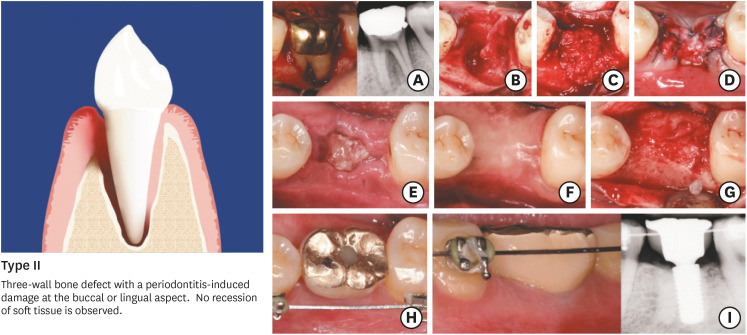
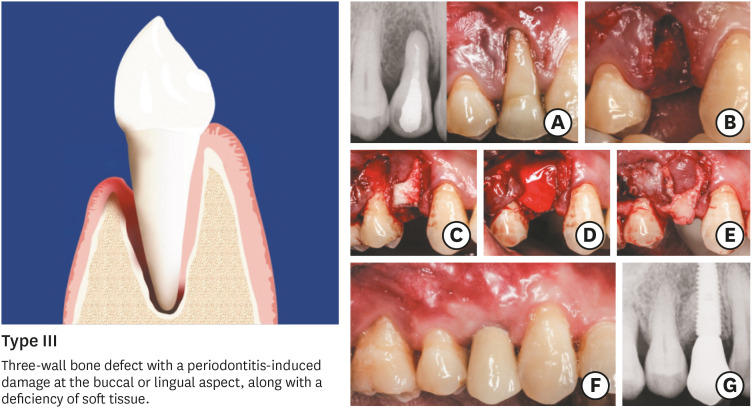
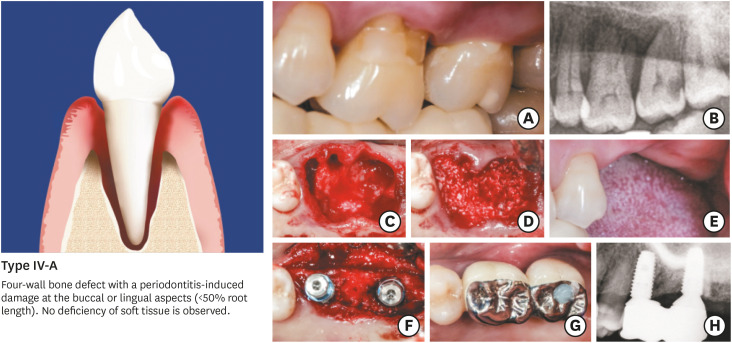
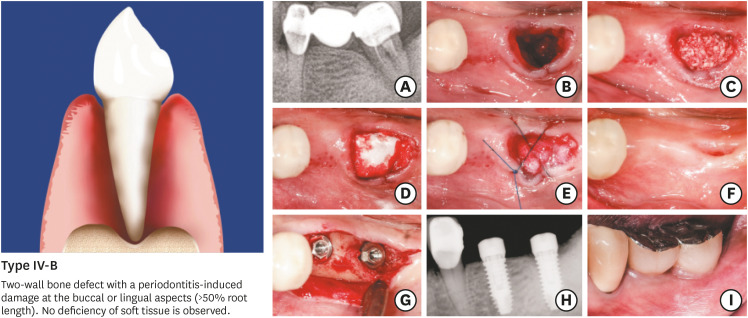
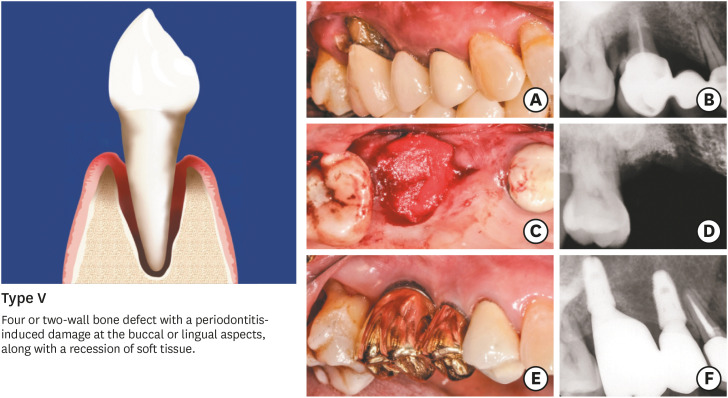
Results: The extraction sockets were classified into 5 types: type I, type II, type III, type IV (A & B), and type V. In this system, the severity of bone and soft tissue breakdown increases from type I to type V, while the reconstruction potential and treatment predictability decrease according to the same sequence of socket types. The retrospective screening of the included extraction sites revealed that most of the sockets assigned to ridge preservation displayed features of type IV (86.87%).
Conclusions: The present article classified different types of commonly observed infected sockets based on diverse levels of ridge destruction. Type IV sockets, featuring an advanced breakdown of alveolar bone, appear to be more frequent than the other socket types.
Keywords: Alveolar ridge augmentation; Classification; Periodontitis; Socket graft; Tooth socket.
Copyright © 2021. Korean Academy of Periodontology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Pietrokovski J, Massler M. Alveolar ridge resorption following tooth extraction. J Prosthet Dent. 1967;17:21–27. - PubMed
-
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23:313–323. - PubMed
-
- Botticelli D, Berglundh T, Lindhe J. Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol. 2004;31:820–828. - PubMed
-
- Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012;23(Suppl 5):1–21. - PubMed
-
- Kim JH, Susin C, Min JH, Suh HY, Sang EJ, Ku Y, et al. Extraction sockets: erratic healing impeding factors. J Clin Periodontol. 2014;41:80–85. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
