

A Simple Classification of Pancreatic Duct Size and Texture Predicts Postoperative Pancreatic Fistula: A classification of the International Study Group of Pancreatic Surgery
- PMID: 33914473
- PMCID: PMC9891297
- DOI: 10.1097/SLA.0000000000004855
A Simple Classification of Pancreatic Duct Size and Texture Predicts Postoperative Pancreatic Fistula: A classification of the International Study Group of Pancreatic Surgery
Abstract
Objective: The aim of this study was to develop a classification system for pancreas-associated risk factors in pancreatoduodenectomy (PD).
Summary background data: Postoperative pancreatic fistula (POPF) is the most relevant PD-associated complication. A simple standardized surgical reporting system based on pancreas-associated risk factors is lacking.
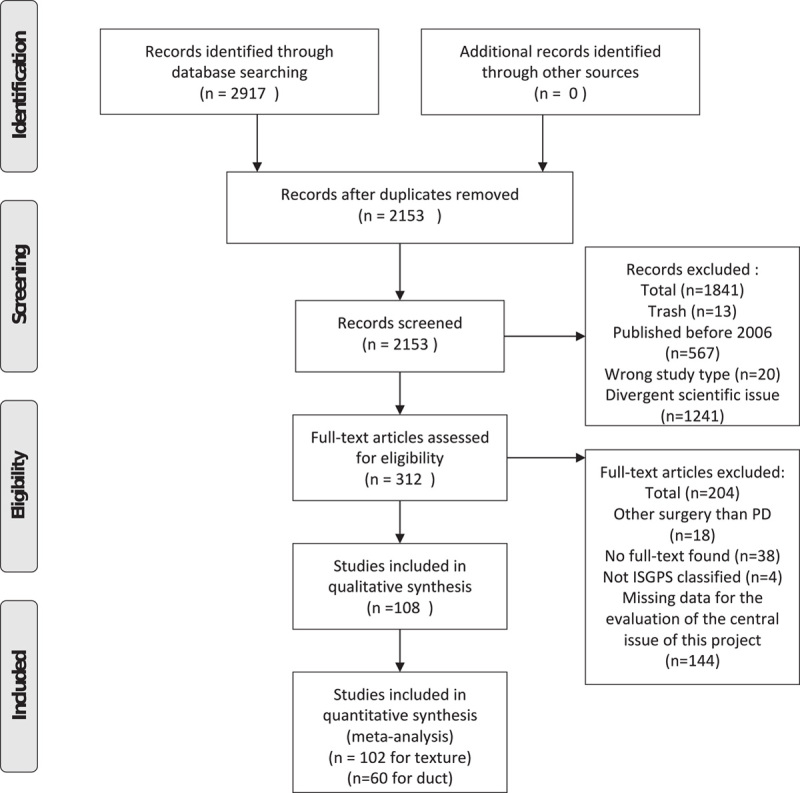
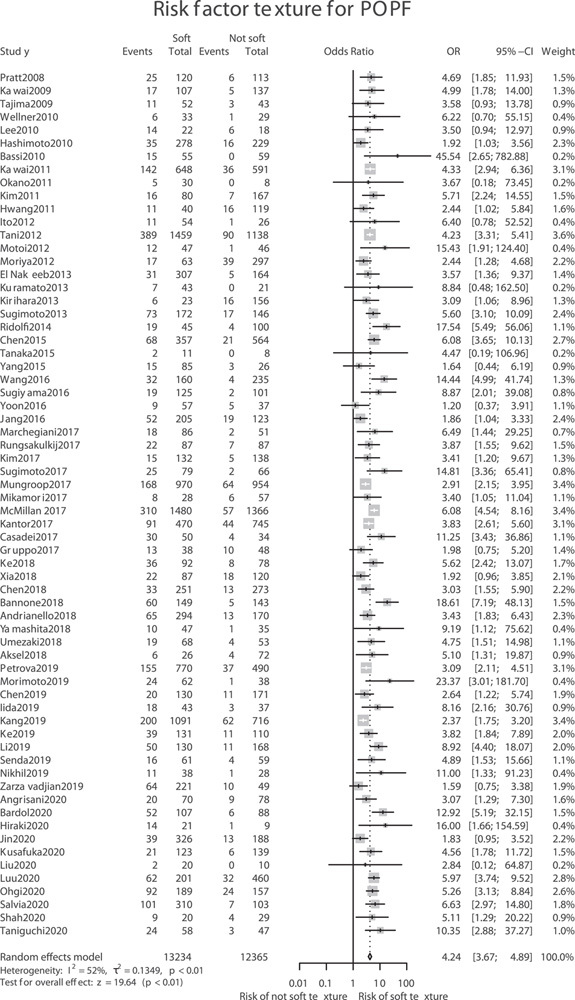
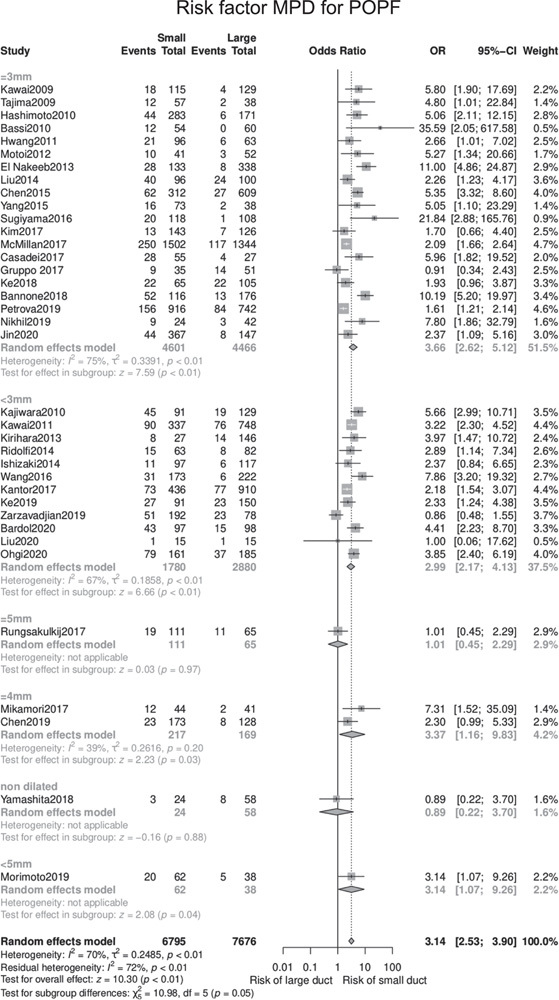
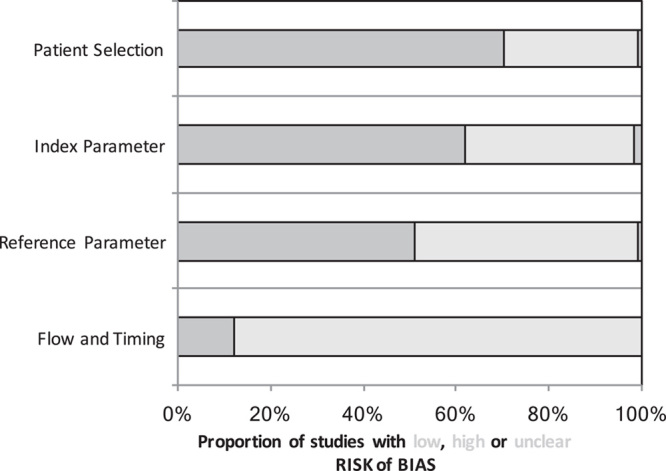
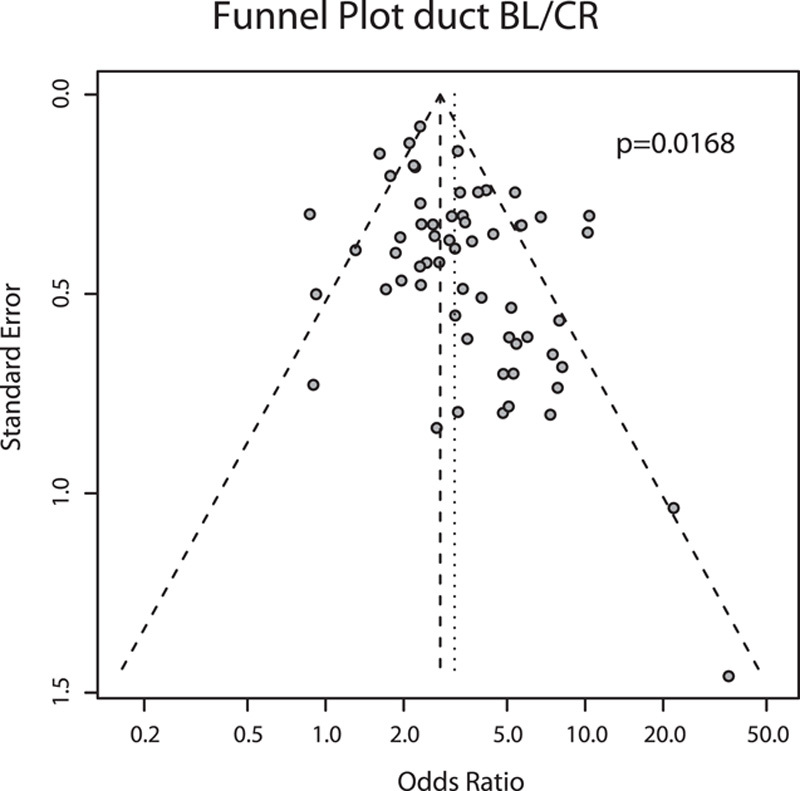
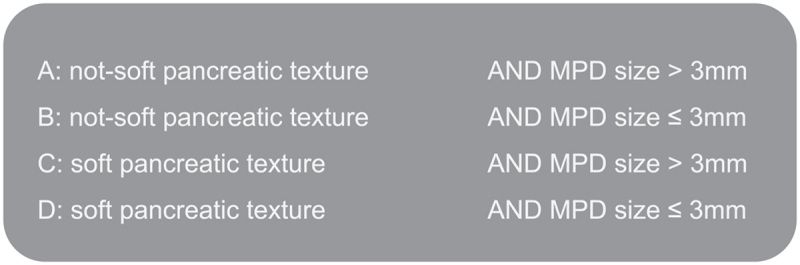
Methods: A systematic literature search was conducted to identify studies investigating clinically relevant (CR) POPF (CR-POPF) and pancreas-associated risk factors after PD. A meta-analysis of CR-POPF rate for texture of the pancreas (soft vs not-soft) and main pancreatic duct (MPD) diameter was performed using the Mantel-Haenszel method. Based on the results, the International Study Group of Pancreatic Surgery (ISGPS) proposes the following classification: A, not-soft (hard) texture and MPD >3 mm; B, not-soft (hard) texture and MPD ≤3 mm; C, soft texture and MPD >3 mm; D, soft texture and MPD ≤3 mm. The classification was evaluated in a multi-institutional, international cohort.
Results: Of the 2917 articles identified, 108 studies were included in the analyses. Soft pancreatic texture was significantly associated with the development of CR-POPF [odds ratio (OR) 4.24, 95% confidence interval (CI) 3.67-4.89, P < 0.01) following PD. Similarly, MPD diameter ≤3 mm significantly increased CR-POPF risk compared with >3 mm diameter MPDs (OR 3.66, 95% CI 2.62-5.12, P < 0.01). The proposed 4-stage system was confirmed in an independent cohort of 5533 patients with CR-POPF rates of 3.5%, 6.2%, 16.6%, and 23.2% for type A-D, respectively ( P < 0.001).
Conclusion: For future pancreatic surgical outcomes studies, the ISGPS recommends reporting these risk factors according to the proposed classification system for better comparability of results.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Comment on article "A Simple Classification of Pancreatic Duct Size and Texture Predicts Postoperative Pancreatic Fistula: A Classification of the International Study Group of Pancreatic Surgery".Ann Surg Open. 2024 Jan 23;5(1):e378. doi: 10.1097/AS9.0000000000000378. eCollection 2024 Mar. Ann Surg Open. 2024. PMID: 38883956 Free PMC article. No abstract available.
References
-
- Mihaljevic AL, Kleeff J, Friess H. Adenocarcinoma of the pancreas. In: Poston GJ, D’Angelica M, Adam R, eds. Surgical Management of Hepatobiliary and Pancreatic Disorders. Informa Healthcare; 2011:380–400.
-
- Witzigmann H, Diener MK, Kienkötter S, et al. . No need for routine drainage after pancreatic head resection: the dual-center, randomized, controlled PANDRA trial (ISRCTN04937707). Ann Surg. 2016;264:528–537. - PubMed
-
- Diener MK, Hüttner FJ, Kieser M, et al. . Partial pancreatoduodenectomy versus duodenum-preserving pancreatic head resection in chronic pancreatitis: the multicentre, randomised, controlled, double-blind ChroPac trial. Lancet Lond Engl. 2017;390:1027–1037. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
