

SARS-CoV-2 testing in North Carolina: Racial, ethnic, and geographic disparities
- PMID: 33915376
- PMCID: PMC8212571
- DOI: 10.1016/j.healthplace.2021.102576
SARS-CoV-2 testing in North Carolina: Racial, ethnic, and geographic disparities
Abstract
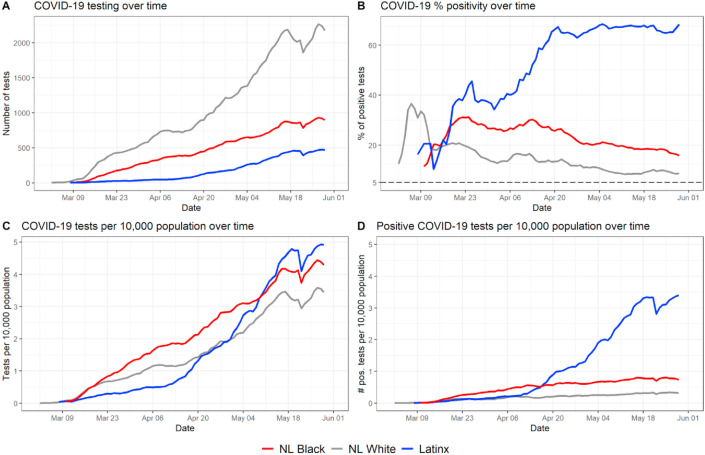
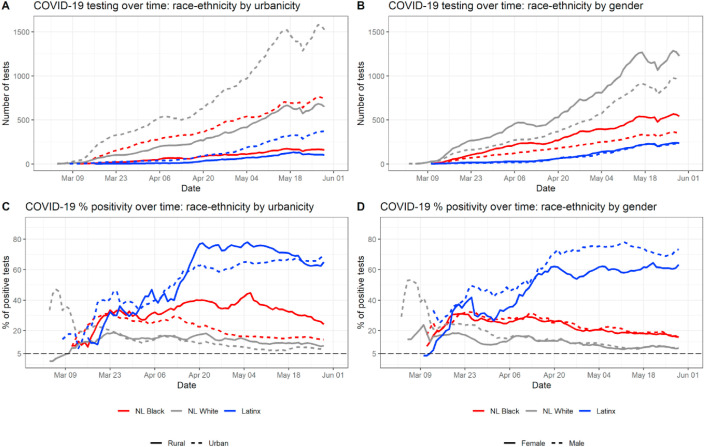
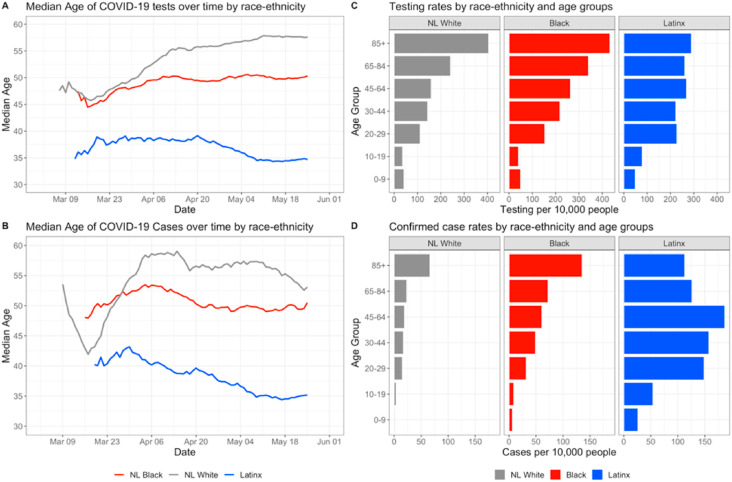
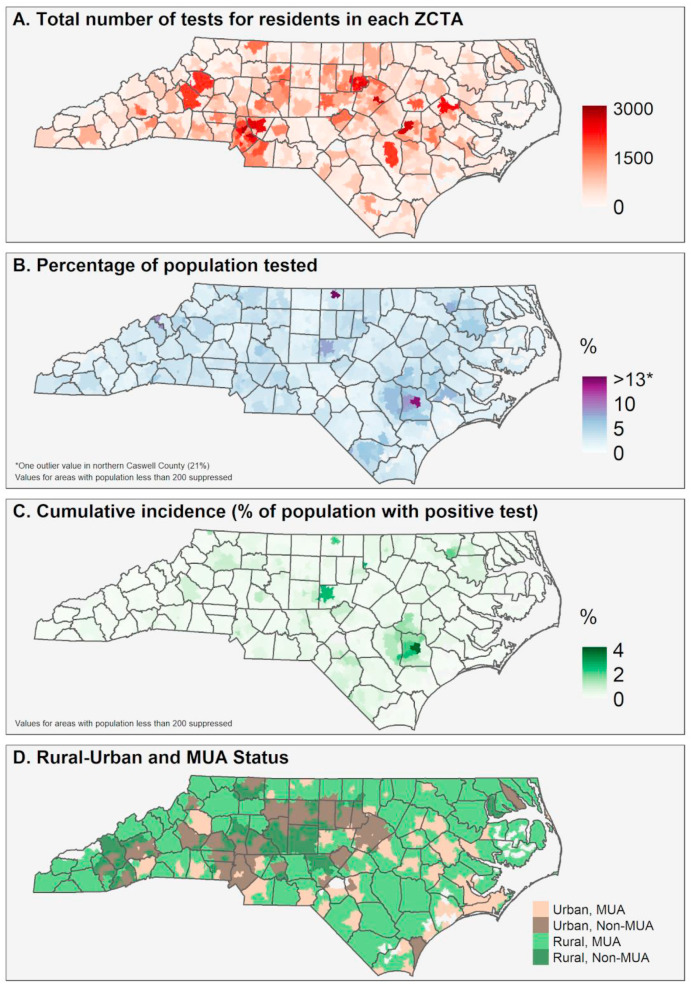
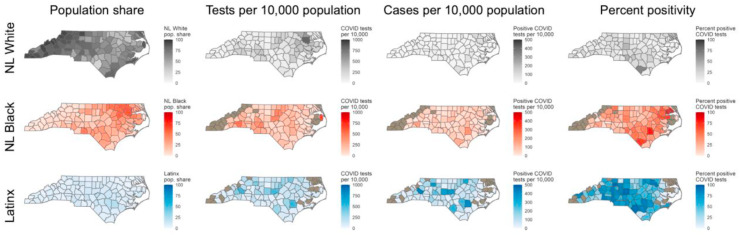
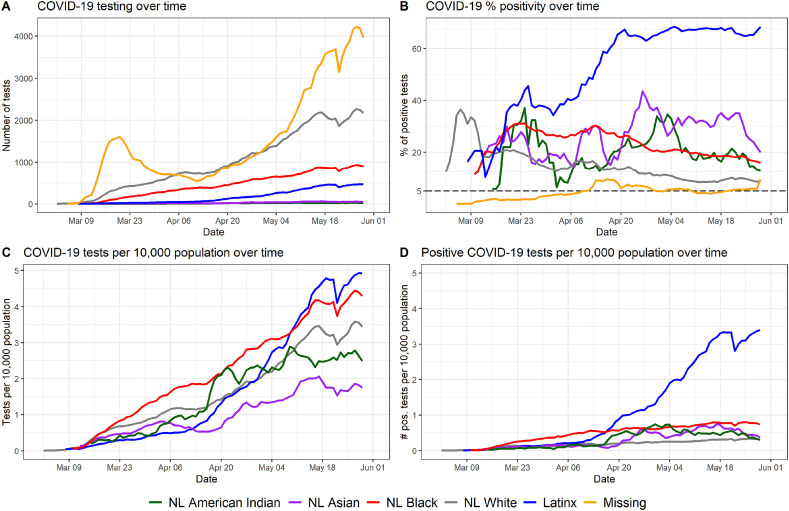
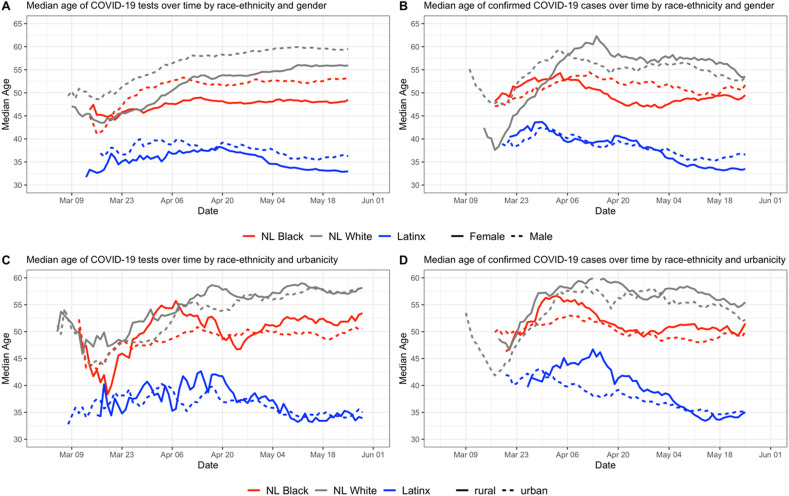
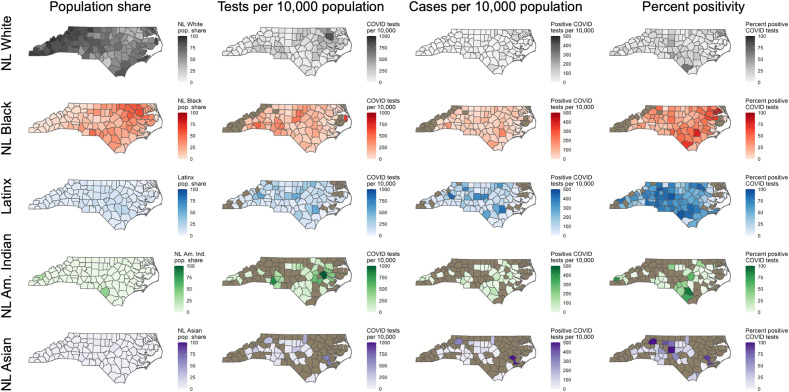
SARS-CoV-2 testing data in North Carolina during the first three months of the state's COVID-19 pandemic were analyzed to determine if there were disparities among intersecting axes of identity including race, Latinx ethnicity, age, urban-rural residence, and residence in a medically underserved area. Demographic and residential data were used to reconstruct patterns of testing metrics (including tests per capita, positive tests per capita, and test positivity rate which is an indicator of sufficient testing) across race-ethnicity groups and urban-rural populations separately. Across the entire sample, 13.1% (38,750 of 295,642) of tests were positive. Within racial-ethnic groups, 11.5% of all tests were positive among non-Latinx (NL) Whites, 22.0% for NL Blacks, and 66.5% for people of Latinx ethnicity. The test positivity rate was higher among people living in rural areas across all racial-ethnic groups. These results suggest that in the first three months of the COVID-19 pandemic, access to COVID-19 testing in North Carolina was not evenly distributed across racial-ethnic groups, especially in Latinx, NL Black and other historically marginalized populations, and further disparities existed within these groups by gender, age, urban-rural status, and residence in a medically underserved area.
Keywords: COVID-19; Healthcare disparity; North Carolina; Public health surveillance; Rural communities; SARS-CoV-2.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures
References
-
- Ajilore O. Rural America is starting to feel the impact of the coronavirus. Center for American Progress. April 28, 2020 https://www.americanprogress.org/issues/economy/reports/2020/04/28/48401...
-
- American Community Survey . US Census Bureau; 2019. 2014-2018 American Community Survey 5-year Estimates.https://www.census.gov/data/developers/data-sets/acs-5year.html
-
- Anselin Luc, Syabri Ibnu, Kho Youngihn. GeoDa: an introduction to spatial data analysis. Geogr. Anal. 2006;38(1):5–22.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
