

Systematic Assessment of Transcriptomic Biomarkers for Immune Checkpoint Blockade Response in Cancer Immunotherapy
- PMID: 33915876
- PMCID: PMC8037221
- DOI: 10.3390/cancers13071639
Systematic Assessment of Transcriptomic Biomarkers for Immune Checkpoint Blockade Response in Cancer Immunotherapy
Abstract
Background: Immune checkpoint blockade (ICB) therapy has yielded successful clinical responses in treatment of a minority of patients in certain cancer types. Substantial efforts were made to establish biomarkers for predicting responsiveness to ICB. However, the systematic assessment of these ICB response biomarkers remains insufficient.
Methods: We collected 22 transcriptome-based biomarkers for ICB response and constructed multiple benchmark datasets to evaluate the associations with clinical response, predictive performance, and clinical efficacy of them in pre-treatment patients with distinct ICB agents in diverse cancers.
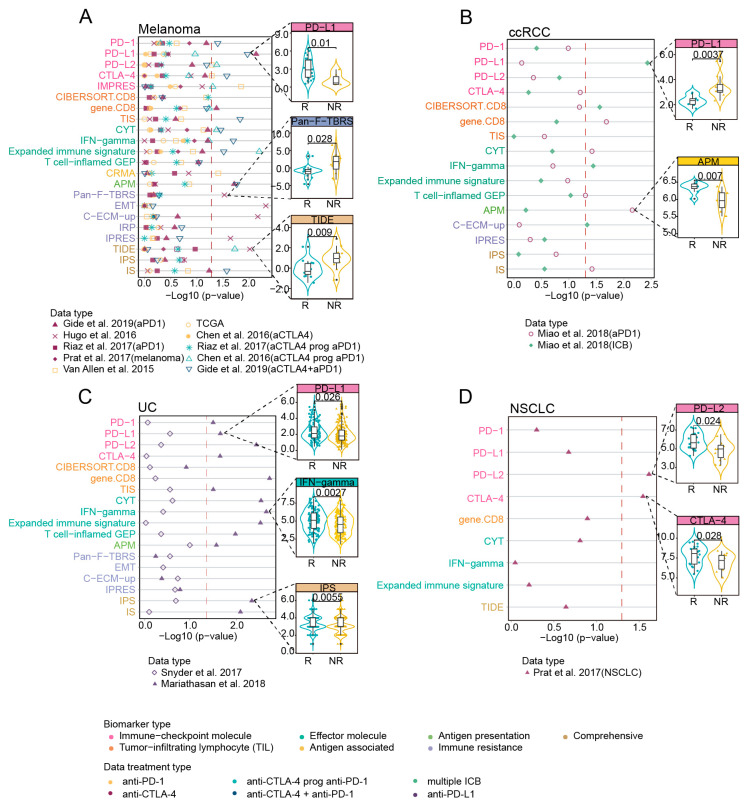
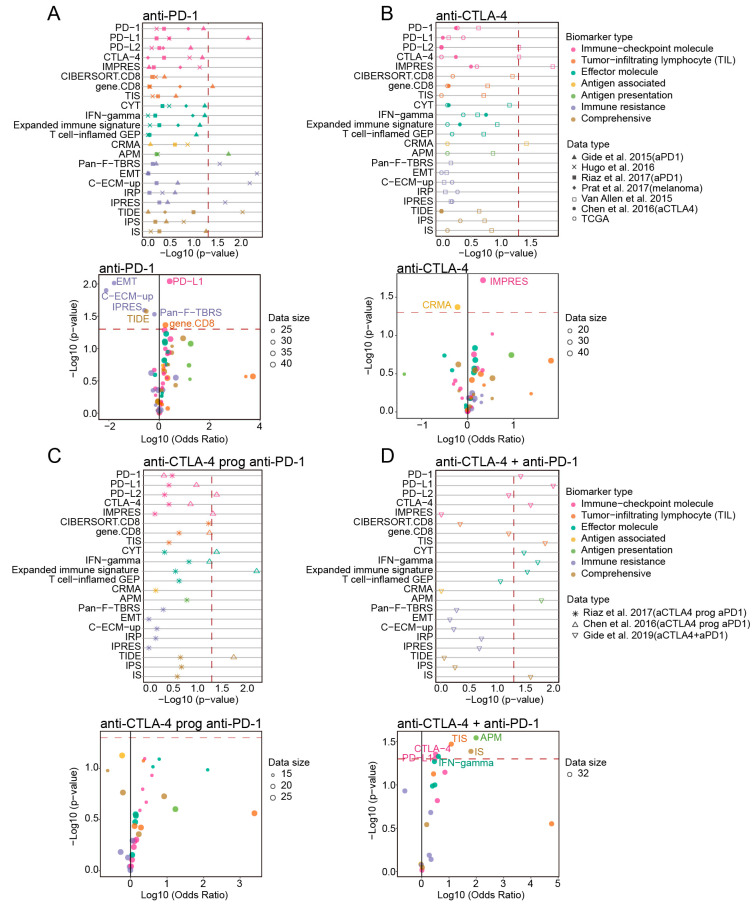
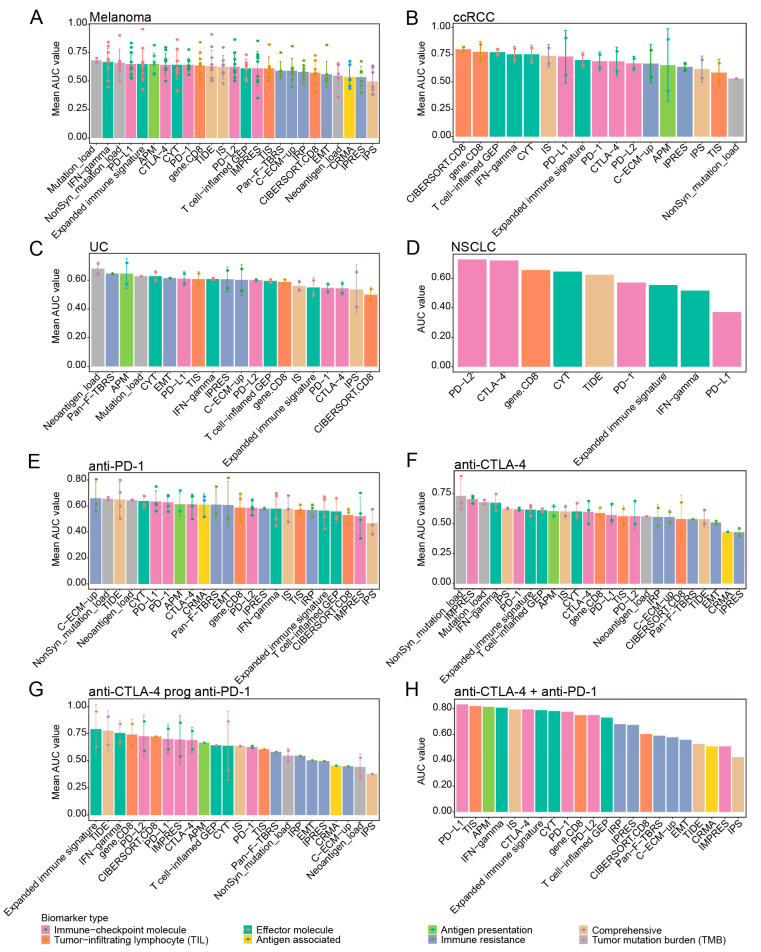
Results: Overall, "Immune-checkpoint molecule" biomarkers PD-L1, PD-L2, CTLA-4 and IMPRES and the "Effector molecule" biomarker CYT showed significant associations with ICB response and clinical outcomes. These immune-checkpoint biomarkers and another immune effector IFN-gamma presented predictive ability in melanoma, urothelial cancer (UC) and clear cell renal-cell cancer (ccRCC). In non-small cell lung cancer (NSCLC), only PD-L2 and CTLA-4 showed preferable correlation with clinical response. Under different ICB therapies, the top-performing biomarkers were usually mutually exclusive in patients with anti-PD-1 and anti-CTLA-4 therapy, and most of biomarkers presented outstanding predictive power in patients with combined anti-PD-1 and anti-CTLA-4 therapy.
Conclusions: Our results show these biomarkers had different performance in predicting ICB response across distinct ICB agents in diverse cancers.
Keywords: comparative analysis; immune checkpoint blockade (ICB); immune response; immunotherapy; transcriptomic biomarkers.
Conflict of interest statement
We declare that we do not have any commercial or associative interest that represents a conflict of interest in connection with the work submitted.
Figures
References
-
- Pitt J.M., Vetizou M., Daillere R., Roberti M.P., Yamazaki T., Routy B., Lepage P., Boneca I.G., Chamaillard M., Kroemer G., et al. Resistance Mechanisms to Immune-Checkpoint Blockade in Cancer: Tumor-Intrinsic and -Extrinsic Factors. Immunity. 2016;44:1255–1269. doi: 10.1016/j.immuni.2016.06.001. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
