

Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project
- PMID: 33916227
- PMCID: PMC8066874
- DOI: 10.3390/microorganisms9040738
Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project
Abstract
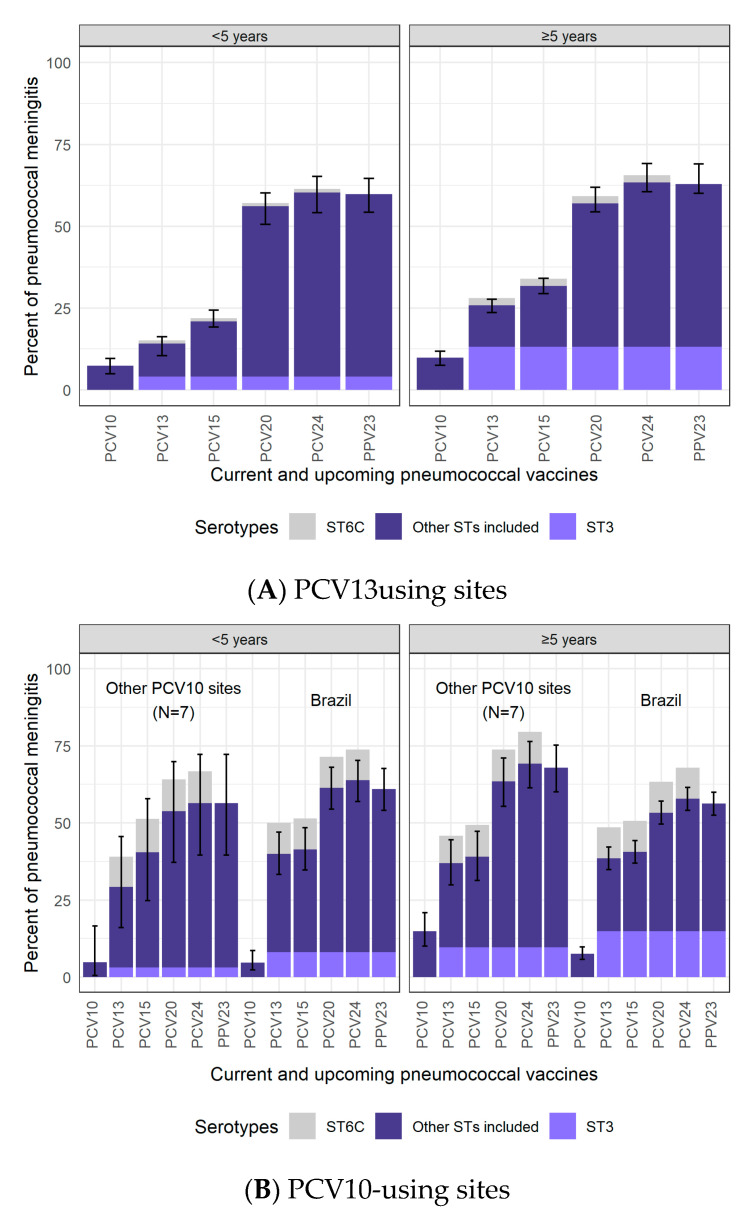
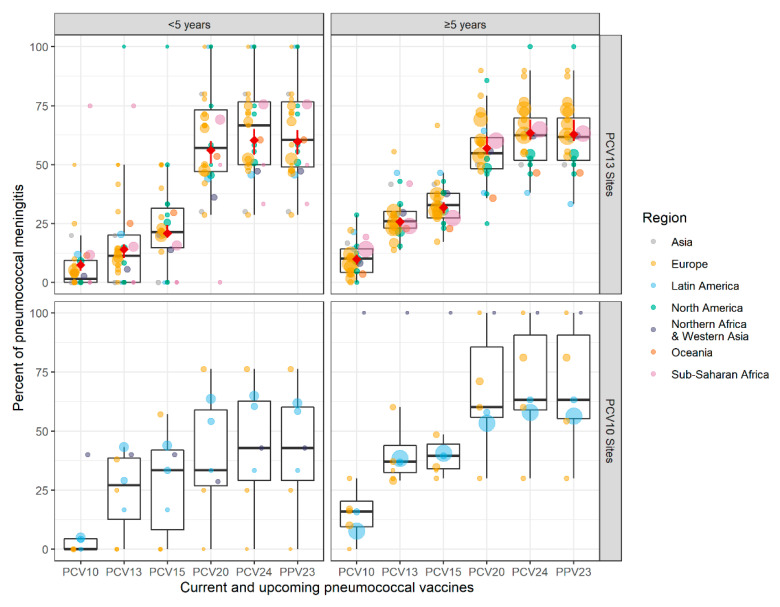
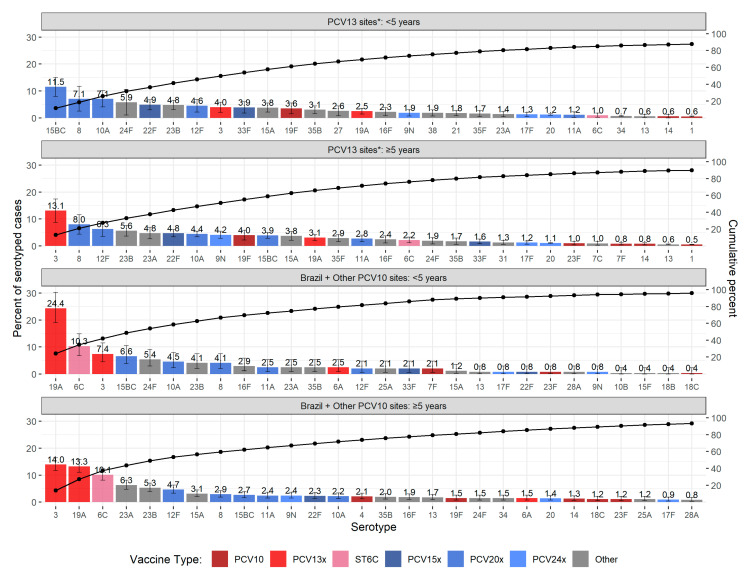
Pneumococcal conjugate vaccine (PCV) introduction has reduced pneumococcal meningitis incidence. The Pneumococcal Serotype Replacement and Distribution Estimation (PSERENADE) project described the serotype distribution of remaining pneumococcal meningitis in countries using PCV10/13 for least 5-7 years with primary series uptake above 70%. The distribution was estimated using a multinomial Dirichlet regression model, stratified by PCV product and age. In PCV10-using sites (N = 8; cases = 1141), PCV10 types caused 5% of cases <5 years of age and 15% among ≥5 years; the top serotypes were 19A, 6C, and 3, together causing 42% of cases <5 years and 37% ≥5 years. In PCV13-using sites (N = 32; cases = 4503), PCV13 types caused 14% in <5 and 26% in ≥5 years; 4% and 13%, respectively, were serotype 3. Among the top serotypes are five (15BC, 8, 12F, 10A, and 22F) included in higher-valency PCVs under evaluation. Other top serotypes (24F, 23B, and 23A) are not in any known investigational product. In countries with mature vaccination programs, the proportion of pneumococcal meningitis caused by vaccine-in-use serotypes is lower (≤26% across all ages) than pre-PCV (≥70% in children). Higher-valency PCVs under evaluation target over half of remaining pneumococcal meningitis cases, but questions remain regarding generalizability to the African meningitis belt where additional data are needed.
Keywords: PCV impact; global; meta-analysis; pneumococcal meningitis; serotype distribution.
Conflict of interest statement
K.H. conducted the study and analyses while working at the Johns Hopkins School of Public Health but is an employee at Pfizer, Inc. as of 26 October 2020. M.D.K. reports grants from Merck, personal fees from Merck, and grants from Pfizer, outside the submitted work. J.C.B. reports funding from Pfizer in the past year, unrelated to the submitted work. M.L. has been a member of advisory boards and has received speaker’s honoraria from Pfizer and Merck. German pneumococcal surveillance has been supported by Pfizer and Merck. S.D. reports grant from Pfizer, outside the submitted work. J.C.S. had received assistance from Pfizer for attending scientific meetings outside the submitted work. K.A. reports a grant from Merck, outside the submitted work. M.C. has previously received a professional fee from Pfizer (Ireland), an unrestricted research grant from Pfizer Ireland (2007–2016), and an Investigator Initiated Reward from Pfizer Ireland in 2018 (W1243730). S.C.G.A. received travel grant from Pfizer. A.M. has received research support to their institution from Pfizer and Merck; honoraria for advisory board membership from GlaxoSmithKline, Merck and Pfizer. S.N.L. performs contract research for GSK, Pfizer, Sanofi Pasteur on behalf of St. George’s University of London but receives no personal remuneration. I.Y. was a member of mRNA-1273 study group and has received funding to her institution to conduct clinical research from BioFire, MedImmune, Regeneron, PaxVax, Pfizer, GSK, Merck, Novavax, Sanofi-Pasteur, and Micron. R.D. has received grants/research support from Pfizer, Merck Sharp and Dohme, and Medimmune; has been a scientific consultant for Pfizer, MeMed, Merck Sharp and Dohme, and Biondvax; had served on advisory boards of Pfizer, Merck Sharp and Dohme, and Biondvax and has been a speaker for Pfizer. L.L.H. reports research grants to her institution from GSK, Pfizer, and Merck. E.V. reports grants from the French public health agency, during the conduct of the study and grants from Pfizer and grants from Merck outside the submitted work. M.H. received an educational grant from Pfizer AG for partial support of this project. However, Pfizer AG had no role in the data analysis and content of the manuscript. N.B.Z. has received investigator-initiated research grants from GlaxoSmithKline, Takeda Pharmaceuticals, Merck, and the Serum Institute of India, all unrelated to this research. N.Mv.S. reports grants and fees for service from Pfizer, fees for service from MSD and GSK, outside the submitted work; in addition, N.Mv.S. has a patent WO 2013/020090 A3 with royalties paid to University of California San Diego (inventors: Nina van Sorge/Victor Nizet). M.C.B. reports lecture fees from MSD outside from submitted work. C.L.B., M.D., has intellectual property in BioFire Diagnostics and receives royalties through the University of Utah. C.L.B. is an advisor to IDbyDNA. M.T. reports grants from GlaxoSmithKline and grants from Pfizer Inc. to the Finnish Institute for Health and Welfare for research projects outside the submitted work, in which she has been a co-investigator. Av.G. as received researching funding from Pfizer (last year 2017, Pfizer Investigator-Initiated Research [IIR] Program IIR WI 194379); they have attended advisory board meetings for Pfizer and Merck. C.M.A. reports grants and personal fees from Pfizer, Qiagen, and BioMerieux and grants from Genomica SAU, outside the submitted work. BL had two research grants from Pfizer on Streptococcus pneumoniae. J.D.K. has received an unrestricted grant-in-aid from Pfizer Canada that supports, in part, the CASPER invasive pneumococcal disease surveillance project. C.G.S. reports grant funding from Pfizer, Merck, and AstraZeneca in the past 3 years. All other authors did not declare any conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Wahl B., O’Brien K.L., Greenbaum A., Majumder A., Liu L., Chu Y., Lukšić I., Nair H., McAllister D.A., Campbell H., et al. Burden of Streptococcus Pneumoniae and Haemophilus Influenzae Type b Disease in Children in the Era of Conjugate Vaccines: Global, Regional, and National Estimates for 2000–2015. Lancet Glob. Health. 2018;6:e744–e757. doi: 10.1016/S2214-109X(18)30247-X. - DOI - PMC - PubMed
-
- Johnson H.L., Deloria-Knoll M., Levine O.S., Stoszek S.K., Hance L.F., Reithinger R., Muenz L.R., O’Brien K.L. Systematic Evaluation of Serotypes Causing Invasive Pneumococcal Disease among Children Under Five: The Pneumococcal Global Serotype Project. PLoS Med. 2010;7:e1000348. doi: 10.1371/journal.pmed.1000348. - DOI - PMC - PubMed
-
- International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health VIEW-Hub. [(accessed on 29 December 2020)]; Available online: https://view-hub.org.
-
- Lucero M., Dulalia V., Nillos L., Williams G., Parreño R., Nohynek H., Riley I., Makela H. Pneumococcal Conjugate Vaccines for Preventing Vaccine-Type Invasive Pneumococcal Disease and Pneumonia with Consolidation on X-ray in Children under Two Years of Age. Cochrane Database Syst. Rev. 2004;4:CD004977. doi: 10.1002/14651858.CD004977. - DOI - PubMed
-
- Cherian T., Cohen M., de Oliveira L., Farrar J.L., Goldblatt D., Knoll M., Moisi J.C., O’Brien K.L., Pilishvili T., Ramakrishnan M., et al. Pneumococcal Conjugate Vaccine (PCV) Review of Impact Evidence (PRIME): Summary of Findings from Systematic Review. Volume 1. WHO; Geneva, Switzerland: 2017. pp. 1–215. Report to Strategic Advisory Group of Experts on Immunization (SAGE) of the World Health Organization.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
