

Hereditary Prostate Cancer: Genes Related, Target Therapy and Prevention
- PMID: 33916521
- PMCID: PMC8038462
- DOI: 10.3390/ijms22073753
Hereditary Prostate Cancer: Genes Related, Target Therapy and Prevention
Abstract
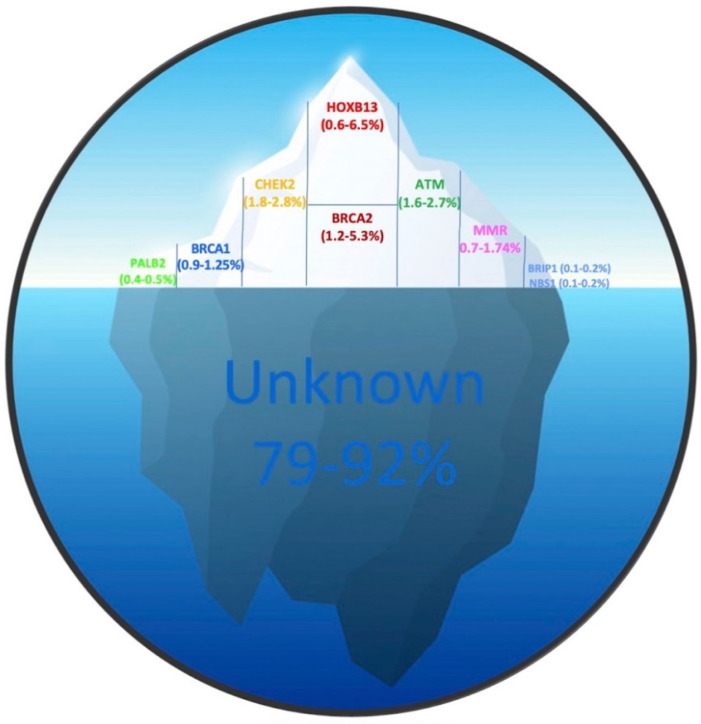
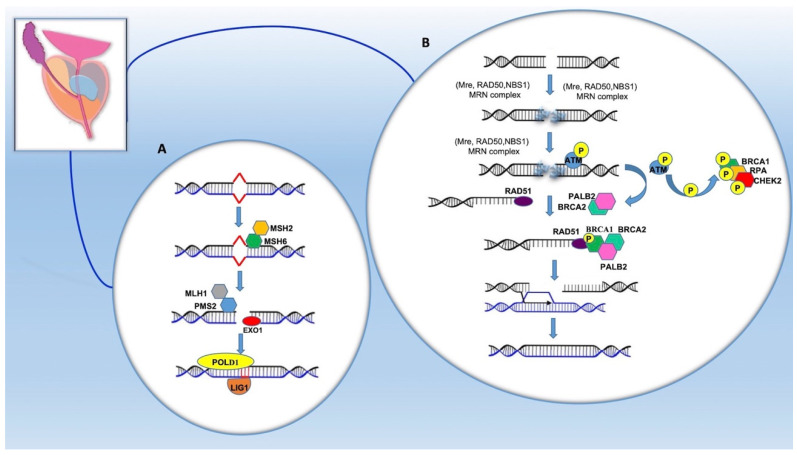
Prostate cancer (PCa) is globally the second most diagnosed cancer type and the most common cause of cancer-related deaths in men. Family history of PCa, hereditary breast and ovarian cancer (HBOC) and Lynch syndromes (LS), are among the most important risk factors compared to age, race, ethnicity and environmental factors for PCa development. Hereditary prostate cancer (HPCa) has the highest heritability of any major cancer in men. The proportion of PCa attributable to hereditary factors has been estimated in the range of 5-15%. To date, the genes more consistently associated to HPCa susceptibility include mismatch repair (MMR) genes (MLH1, MSH2, MSH6, and PMS2) and homologous recombination genes (BRCA1/2, ATM, PALB2, CHEK2). Additional genes are also recommended to be integrated into specific research, including HOXB13, BRP1 and NSB1. Importantly, BRCA1/BRCA2 and ATM mutated patients potentially benefit from Poly (ADP-ribose) polymerase PARP inhibitors, through a mechanism of synthetic lethality, causing selective tumor cell cytotoxicity in cell lines. Moreover, the detection of germline alterations in MMR genes has therapeutic implications, as it may help to predict immunotherapy benefits. Here, we discuss the current knowledge of the genetic basis for inherited predisposition to PCa, the potential target therapy, and the role of active surveillance as a management strategy for patients with low-risk PCa. Finally, the current PCa guideline recommendations are reviewed.
Keywords: genetic testing; genotype–phenotype correlation; hereditary prostate cancer; surveillance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
