

Mycotic Keratitis-A Global Threat from the Filamentous Fungi
- PMID: 33916767
- PMCID: PMC8066744
- DOI: 10.3390/jof7040273
Mycotic Keratitis-A Global Threat from the Filamentous Fungi
Abstract
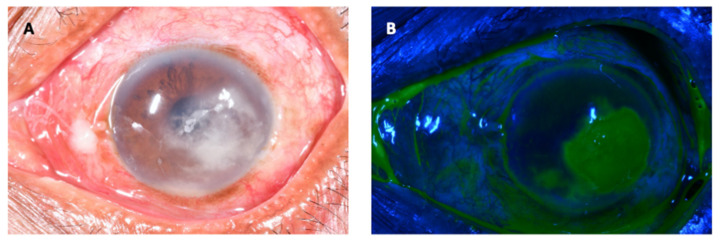
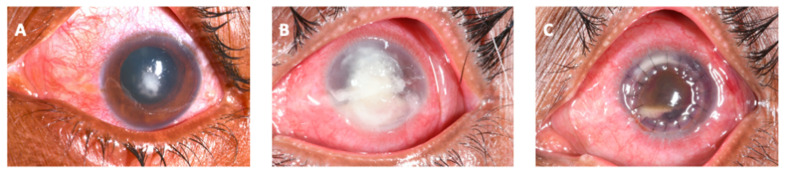
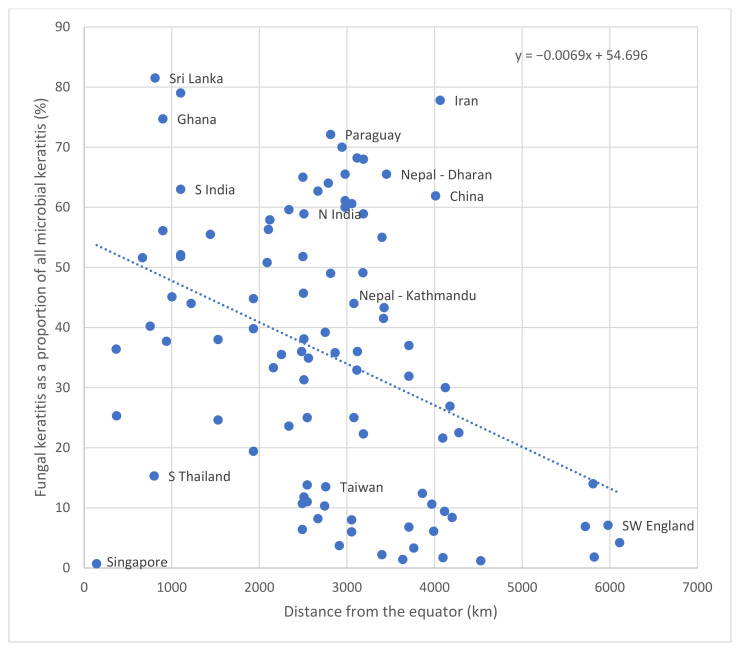
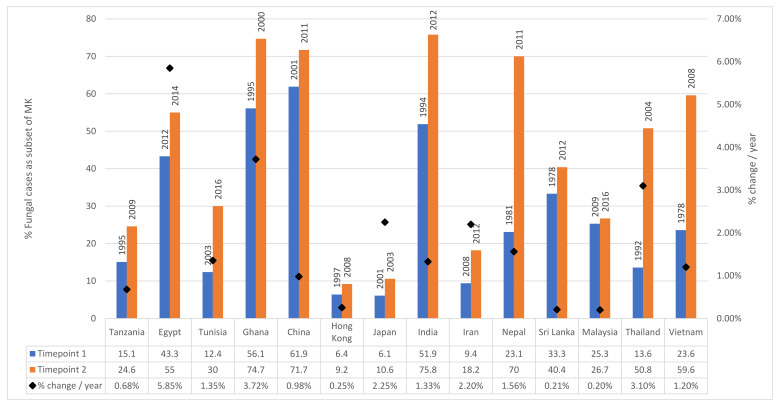
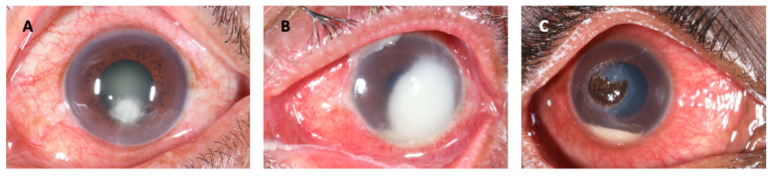
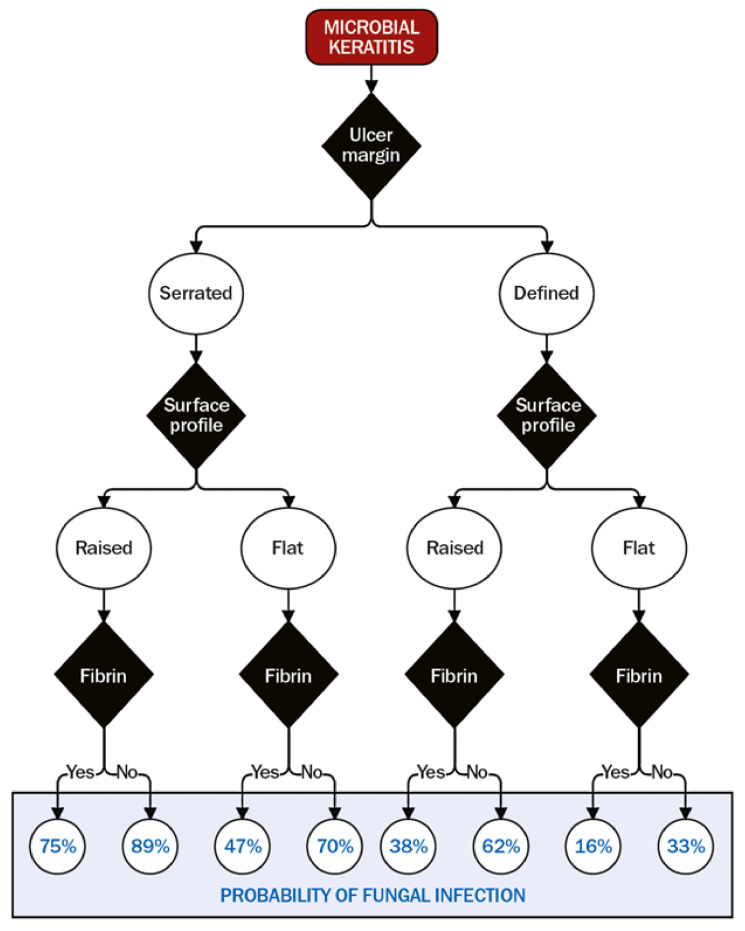
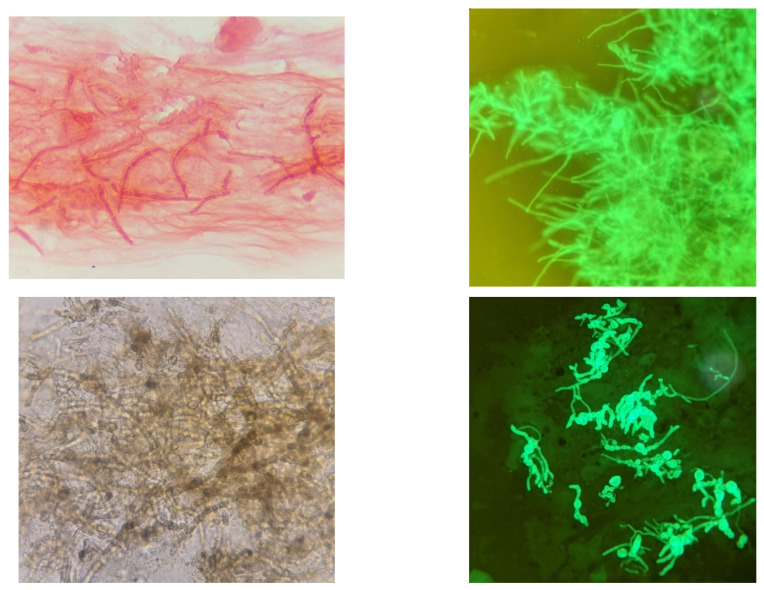
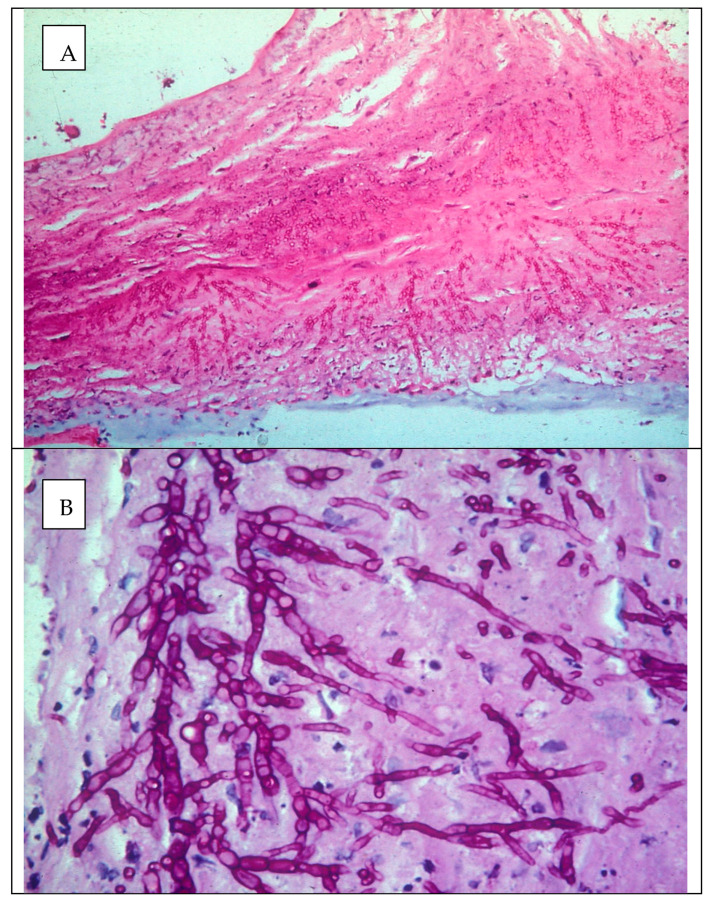
Mycotic or fungal keratitis (FK) is a sight-threatening disease, caused by infection of the cornea by filamentous fungi or yeasts. In tropical, low and middle-income countries, it accounts for the majority of cases of microbial keratitis (MK). Filamentous fungi, in particular Fusarium spp., the aspergilli and dematiaceous fungi, are responsible for the greatest burden of disease. The predominant risk factor for filamentous fungal keratitis is trauma, typically with organic, plant-based material. In developed countries, contact lens wear and related products are frequently implicated as risk factors, and have been linked to global outbreaks of Fusarium keratitis in the recent past. In 2020, the incidence of FK was estimated to be over 1 million cases per year, and there is significant geographical variation; accounting for less than 1% of cases of MK in some European countries to over 80% in parts of south and south-east Asia. The proportion of MK cases is inversely correlated to distance from the equator and there is emerging evidence that the incidence of FK may be increasing. Diagnosing FK is challenging; accurate diagnosis relies on reliable microscopy and culture, aided by adjunctive tools such as in vivo confocal microscopy or PCR. Unfortunately, these facilities are infrequently available in areas most in need. Current topical antifungals are not very effective; infections can progress despite prompt treatment. Antifungal drops are often unavailable. When available, natamycin is usually first-line treatment. However, infections may progress to perforation in ~25% of cases. Future work needs to be directed at addressing these challenges and unmet needs. This review discusses the epidemiology, clinical features, diagnosis, management and aetiology of FK.
Keywords: Aspergillus; Fusarium; blindness; dematiaceous fungi; epidemiology; fungal keratitis; microbial keratitis; microbiology; mycotic keratitis.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures



References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
