

Mild Head Trauma: Is Antiplatelet Therapy a Risk Factor for Hemorrhagic Complications?
- PMID: 33917141
- PMCID: PMC8067857
- DOI: 10.3390/medicina57040357
Mild Head Trauma: Is Antiplatelet Therapy a Risk Factor for Hemorrhagic Complications?
Abstract
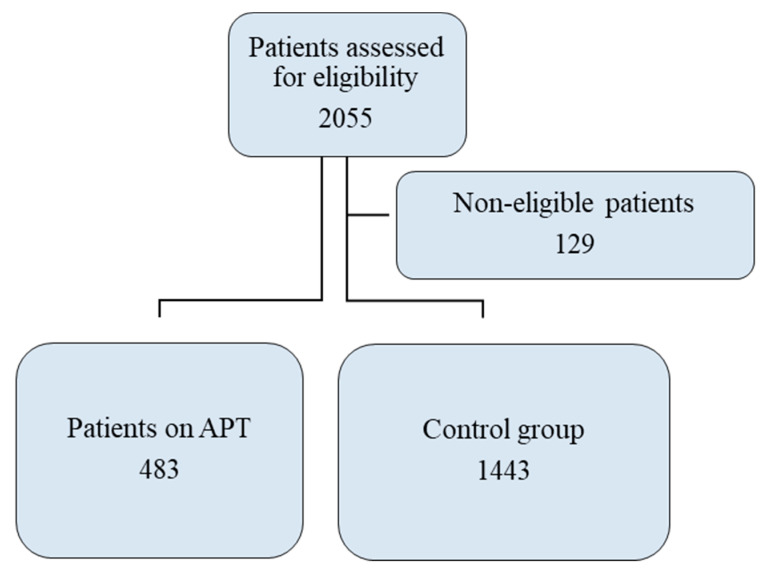
Background and objectives: In patients who receive antiplatelet therapy (APT), the bleeding risk profile after mild head trauma (MHT) still needs clarification. Some studies have demonstrated an association with bleeding risk, whereas others have not. We studied the population of our level II emergency department (ED) trauma center to determine the risk of bleeding in patients receiving APT and whether bleeding results not from antiplatelet agents but rather from age. We assessed the bleeding risk, the incidence of intracranial hemorrhage (ICH) that necessitated hospitalization for observation, the need for cranial neurosurgery, the severity of the patient's condition at discharge, and the frequency of ED revisits for head trauma in patients receiving APT. Materials and Methods: This retrospective single-center study included 483 patients receiving APT who were in the ED for MHT in 2019. The control group consisted of 1443 patients in the ED with MHT over the same period who were not receiving APT or anticoagulant therapy. Our ED diagnostic therapeutic protocol mandates both triage and the medical examination to identify patients with MHT who are taking any anticoagulant or APT. Results: APT was not significantly associated with bleeding risk (p > 0.05); as a risk factor, age was significantly associated with the risk of bleeding, even after adjustment for therapy. Patients receiving APT had a greater need of surgery (1.2% vs. 0.4%; p < 0.0001) and a higher rate of hospitalization (52.9% vs. 37.4%; p < 0.0001), and their clinical condition was more severe (evaluated according to the exit code value on a one-dimensional quantitative five-point numerical scale) at the time of discharge (p = 0.013). The frequency of ED revisits due to head trauma did not differ between the two groups. Conclusions: The risk of bleeding in patients receiving APT who had MHT was no higher than that in the control group. However, the clinical condition of patients receiving APT, including hospital admission for ICH monitoring and cranial neurosurgical interventions, was more severe.
Keywords: antiplatelet therapy; bleeding risk; cranial neurosurgical interventions; emergency department; hospital admission; intracranial hemorrhage; mild head trauma; minor head injury.
Conflict of interest statement
The authors declare no conflict of interest.
References
-
- Bouida W., Marghli S., Souissi S., Ksibi H., Methammem M., Haguiga H., Khedher S., Boubaker H., Beltaief K., Grissa M.H., et al. Prediction Value of the Canadian CT Head Rule and the New Orleans Criteria for Positive Head CT Scan and Acute Neurosurgical Procedures in Minor Head Trauma: A Multicenter External Validation Study. Ann. Emerg. Med. 2013;61:521–527. doi: 10.1016/j.annemergmed.2012.07.016. - DOI - PubMed
-
- Jagoda A.S., Bazarian J.J., Bruns J.J., Cantrill S.V., Gean A.D., Howard P.K., Ghajar J., Riggio S., Wright D.W., Wears R.L., et al. Clinical Policy: Neuroimaging and Decisionmaking in Adult Mild Traumatic Brain Injury in the Acute Setting. Ann. Emerg. Med. 2008;52:714–748. doi: 10.1016/j.annemergmed.2008.08.021. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
