

Successive Osteosarcoma Relapses after the First Line O2006/Sarcome-09 Trial: What Can We Learn for Further Phase-II Trials?
- PMID: 33918346
- PMCID: PMC8038261
- DOI: 10.3390/cancers13071683
Successive Osteosarcoma Relapses after the First Line O2006/Sarcome-09 Trial: What Can We Learn for Further Phase-II Trials?
Abstract
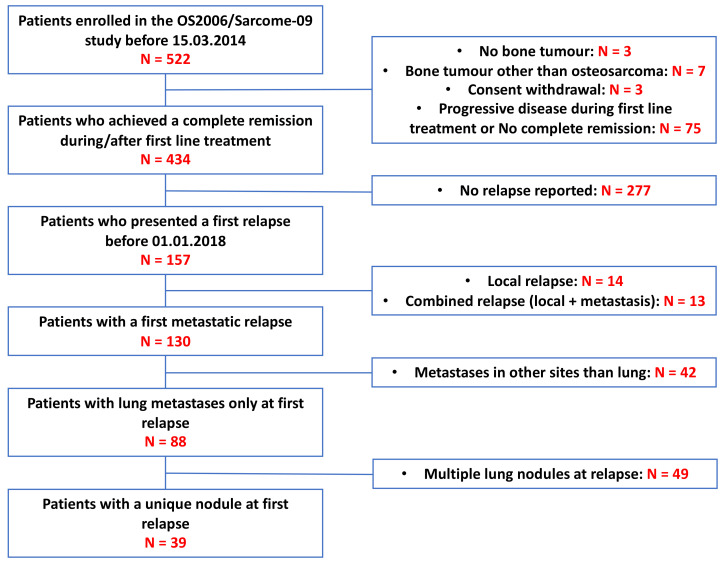
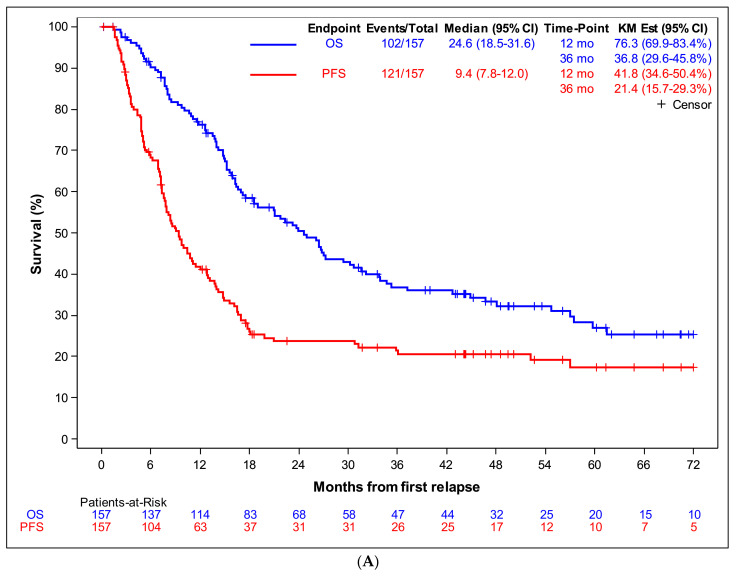
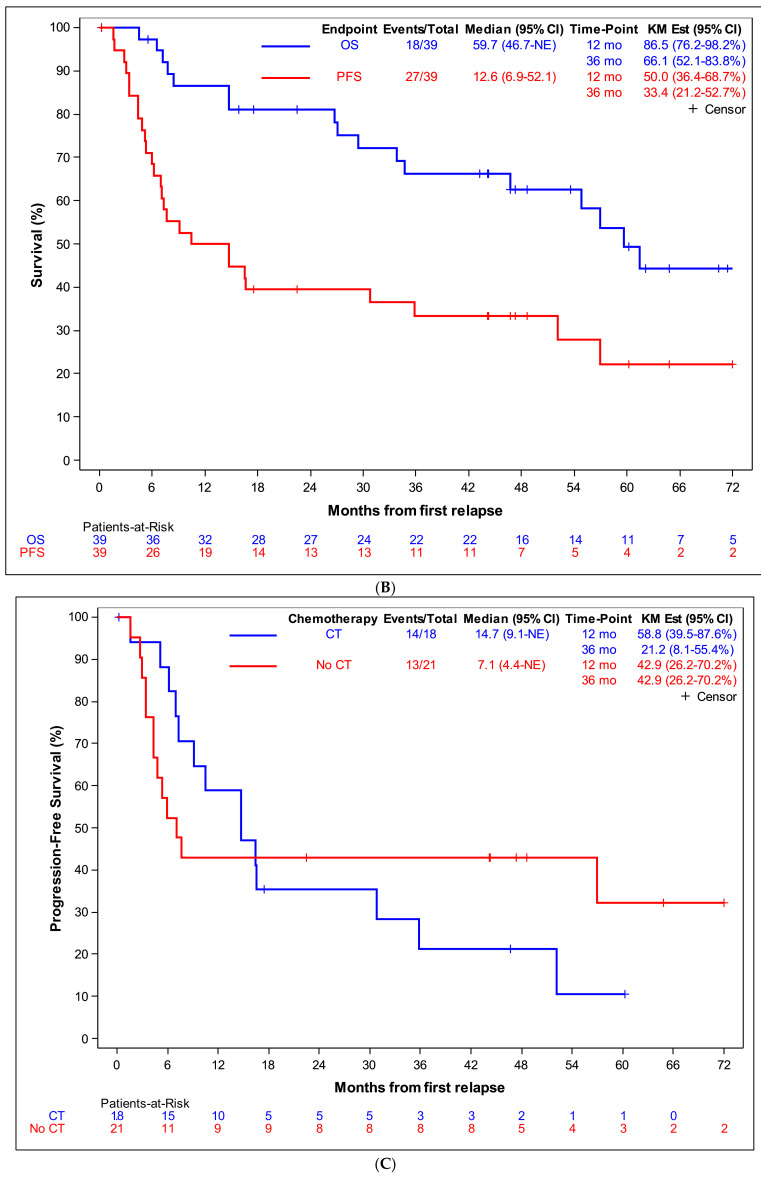
The purpose was to describe first and subsequent relapses in patients from the OS2006/Sarcome-09 trial, to help future trial design. We prospectively collected and analysed relapse data of all French patients included in the OS2006/Sarcome-09 trial, who had achieved a first complete remission. 157 patients experienced a first relapse. The median interval from diagnosis to relapse was 1.7 year (range 0.5-7.6). The first relapse was metastatic in 83% of patients, and disease was not measurable according to RECIST 1.1 criteria in 23%. Treatment consisted in systemic therapy (74%) and surgical resection (68%). A quarter of the patients were accrued in a phase-II clinical trial. A second complete remission was obtained for 79 patients. Most of them had undergone surgery (76/79). The 3-year progression-free and overall survival rates were 21% and 37%, respectively. In patients who achieved CR2, the 3y-PFS and OS rates were 39% and 62% respectively. Individual correlation between subsequent PFS durations was poor. For osteosarcoma relapses, we recommend randomised phase-II trials, open to patients from all age categories (children, adolescents, adults), not limited to patients with measurable disease (but stratified according to disease status), with PFS as primary endpoint, response rate and surgical CR as secondary endpoints.
Keywords: RECIST; metastasis; osteosarcoma; phase-II trial; recurrence/relapse.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Desandes E., Stark D.P. Epidemiology of Adolescents and Young Adults with Cancer in Europe. Prog. Tumor. Res. 2016;43:1–15. - PubMed
-
- Piperno-Neumann S., Le Deley M.C., Rédini F., Pacquement H., Marec-Bérard P., Petit P., Brisse H., Lervat C., Gentet J.C., Entz-Werlé N., et al. Zoledronate in combination with chemotherapy and surgery to treat osteosarcoma (OS2006): A randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016;17:1070–1080. doi: 10.1016/S1470-2045(16)30096-1. - DOI - PubMed
-
- Smeland S., Bielack S.S., Whelan J., Bernstein M., Hogendoorn P., Krailo M.D., Gorlick R., Janeway K.A., Ingleby F.C., Anninga J., et al. Survival and prognosis with osteosarcoma: Outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur. J. Cancer. 2019;109:36–50. doi: 10.1016/j.ejca.2018.11.027. - DOI - PMC - PubMed
-
- Friebele J.C., Peck J., Pan X., Abdel-Rasoul M., Mayerson J.L. Osteosarcoma: A Meta-Analysis and Review of the Literature. Am. J. Orthop. 2015;44:547–553. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
