

Screening of FDA-Approved Drugs Using a MERS-CoV Clinical Isolate from South Korea Identifies Potential Therapeutic Options for COVID-19
- PMID: 33918958
- PMCID: PMC8069929
- DOI: 10.3390/v13040651
Screening of FDA-Approved Drugs Using a MERS-CoV Clinical Isolate from South Korea Identifies Potential Therapeutic Options for COVID-19
Abstract
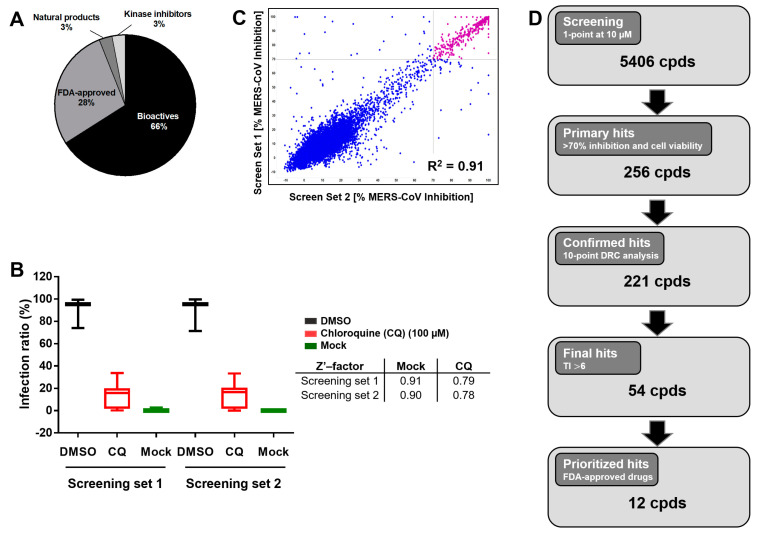
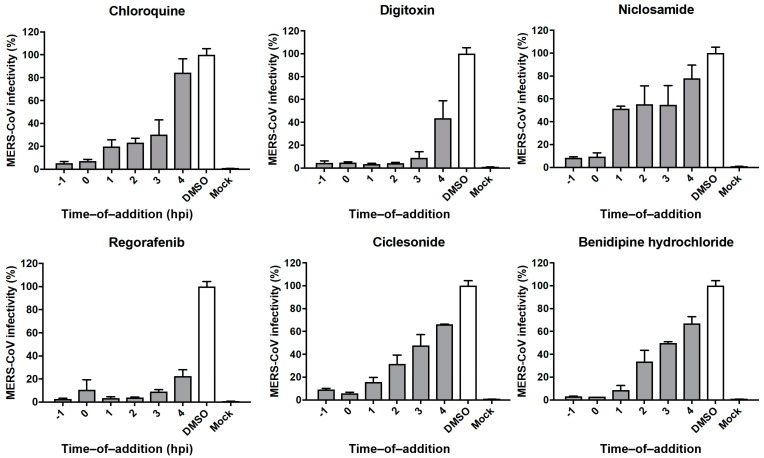
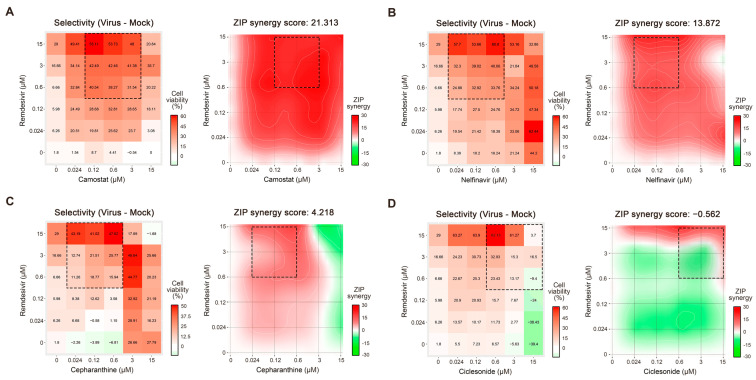
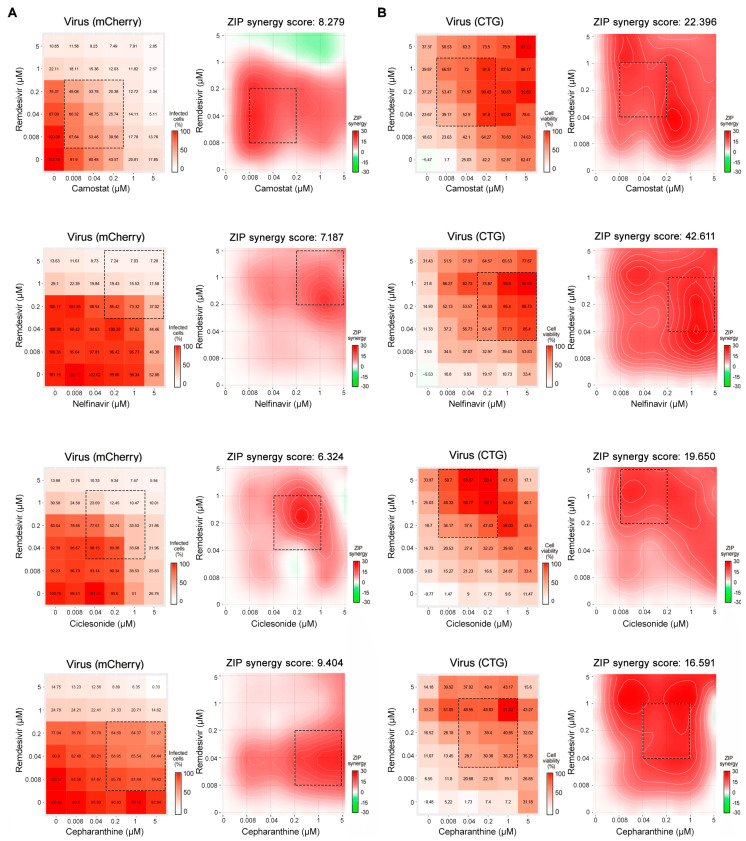
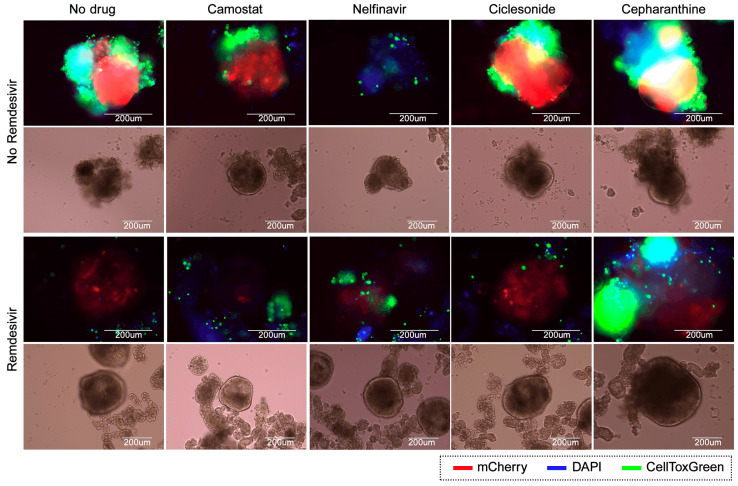
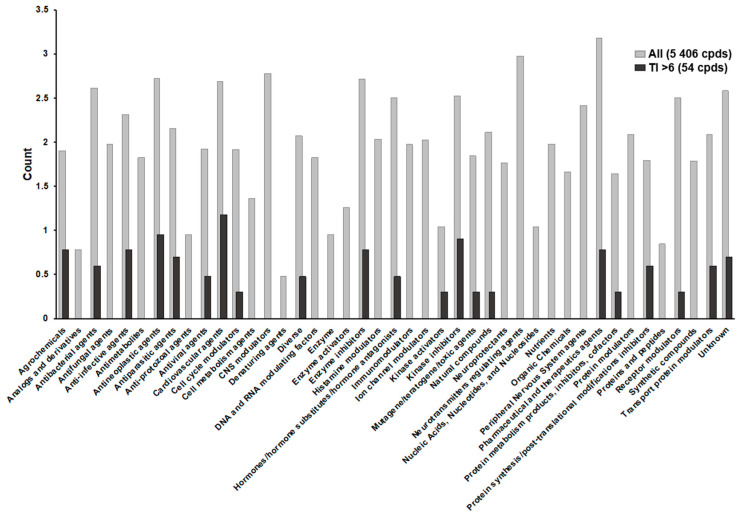
Therapeutic options for coronaviruses remain limited. To address this unmet medical need, we screened 5406 compounds, including United States Food and Drug Administration (FDA)-approved drugs and bioactives, for activity against a South Korean Middle East respiratory syndrome coronavirus (MERS-CoV) clinical isolate. Among 221 identified hits, 54 had therapeutic indexes (TI) greater than 6, representing effective drugs. The time-of-addition studies with selected drugs demonstrated eight and four FDA-approved drugs which acted on the early and late stages of the viral life cycle, respectively. Confirmed hits included several cardiotonic agents (TI > 100), atovaquone, an anti-malarial (TI > 34), and ciclesonide, an inhalable corticosteroid (TI > 6). Furthermore, utilizing the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), we tested combinations of remdesivir with selected drugs in Vero-E6 and Calu-3 cells, in lung organoids, and identified ciclesonide, nelfinavir, and camostat to be at least additive in vitro. Our results identify potential therapeutic options for MERS-CoV infections, and provide a basis to treat coronavirus disease 2019 (COVID-19) and other coronavirus-related illnesses.
Keywords: COVID-19; FDA-approved drugs; Middle East respiratory syndrome coronavirus; clinical isolate; drug combinations; drug repurposing; high-content screening; lung organoids; pandemic; severe acute respiratory syndrome coronavirus disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization Summary of Probably SARS Cases with Onset of Illness from 1 November 2002 to 31 July 2003. [(accessed on 16 November 2020)]; Available online: https://www.who.int/publications/m/item/summary-of-probable-sars-cases-w....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
