

Primary Hyperparathyroidism: A Narrative Review of Diagnosis and Medical Management
- PMID: 33918966
- PMCID: PMC8068862
- DOI: 10.3390/jcm10081604
Primary Hyperparathyroidism: A Narrative Review of Diagnosis and Medical Management
Abstract
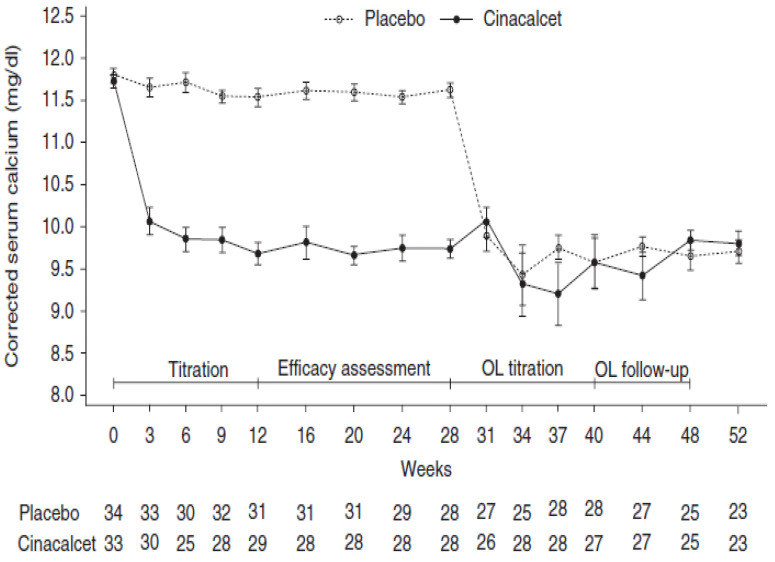
Primary hyperparathyroidism (PHPT) is the most common cause of hypercalcemia in the outpatient setting. Symptomatic presentation includes non-specific signs and symptoms of hypercalcemia, skeletal fragility, nephrolithiasis and nephrocalcinosis. The majority of individuals present at an asymptomatic stage following routine biochemical screening, without any signs or symptoms of calcium or parathyroid hormone (PTH) excess or target organ damage. Indications for surgery have recently been revised as published in recent guidelines and consensus statements. Parathyroidectomy is advised in patients younger than 50 years old and in the presence of either significant hypercalcemia, impaired renal function, renal stones or osteoporosis. Surgery is always appropriate in suitable surgical candidates, however, medical management may be considered in those with mild asymptomatic disease, contraindications to surgery or failed previous surgical intervention. We summarized the optimal medical interventions available in the care of PHPT patients not undergoing parathyroidectomy. Calcium and vitamin D intake should be optimized. Antiresorptive therapy may be used for skeletal protection in patients with an increased fracture risk. Cinacalcet, a calcimimetic agent, has been shown to effectively lower serum calcium and PTH levels. The effect of medical treatment on the reduction in fracture risk is unknown and should be the focus of future research.
Keywords: bisphosphonates; cinacalcet; denosumab; estrogen; primary hyperparathyroidism; raloxifene.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Khan A.A., Hanley D.A., Rizzoli R., Bollerslev J., Young J., Rejnmark L., Thakker R., D’Amour P., Paul T., Van Uum S., et al. Primary hyperparathyroidism: Review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos. Int. 2017;28:1–19. doi: 10.1007/s00198-016-3716-2. - DOI - PMC - PubMed
-
- Press D.M., Siperstein A.E., Berber E., Shin J.J., Metzger R., Jin J., Monteiro R., Mino J.S., Swagel W., Mitchell J.C. The prevalence of undiagnosed and unrecognized primary hyperparathyroidism: A population-based analysis from the electronic medical record. Surgery. 2013;154:1232–1238. doi: 10.1016/j.surg.2013.06.051. - DOI - PubMed
-
- Silverberg S.J., Clarke B.L., Peacock M., Bandeira F., Boutroy S., Cusano N.E., Dempster D., Lewiecki E.M., Liu J.-M., Minisola S., et al. Current issues in the presentation of asymptomatic primary hyperparathyroidism: Proceedings of the fourth international workshop. J. Clin. Endocrinol. Metab. 2014;99:3580–3594. doi: 10.1210/jc.2014-1415. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
