

Bromodomain and Extraterminal Protein Inhibitor, Apabetalone (RVX-208), Reduces ACE2 Expression and Attenuates SARS-Cov-2 Infection In Vitro
- PMID: 33919584
- PMCID: PMC8072876
- DOI: 10.3390/biomedicines9040437
Bromodomain and Extraterminal Protein Inhibitor, Apabetalone (RVX-208), Reduces ACE2 Expression and Attenuates SARS-Cov-2 Infection In Vitro
Abstract
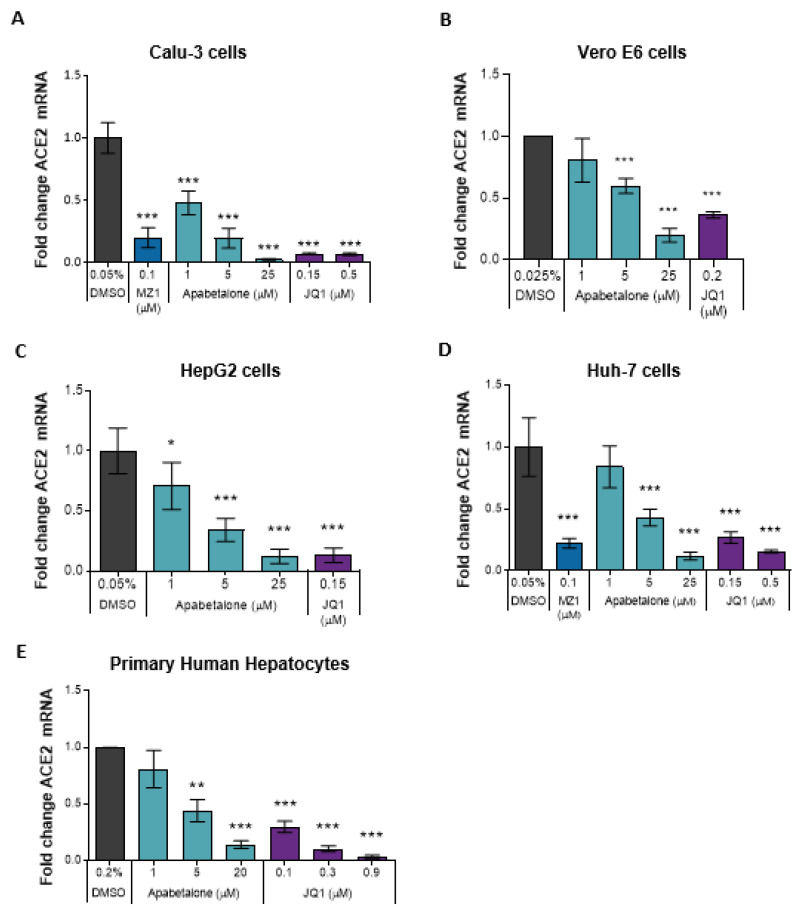
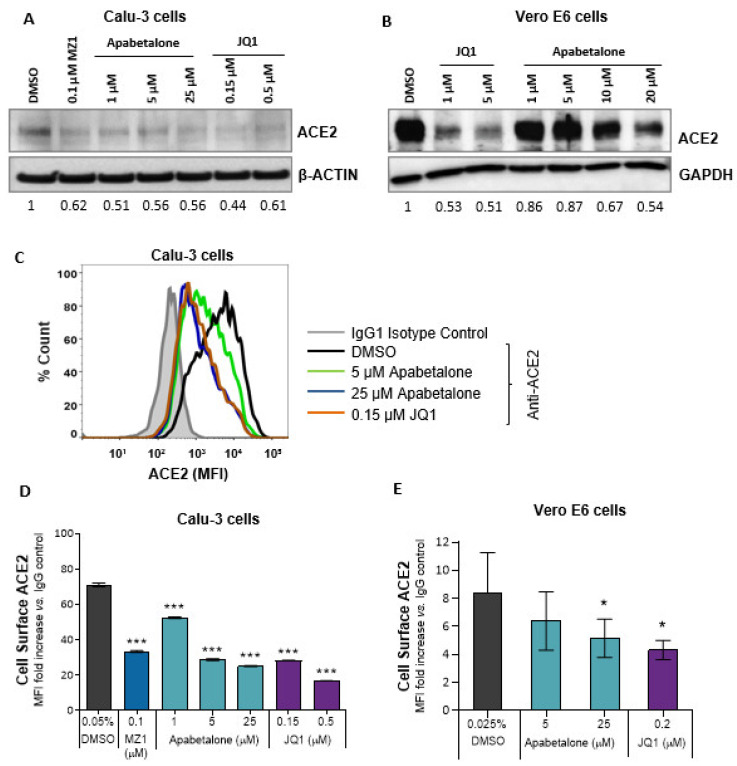
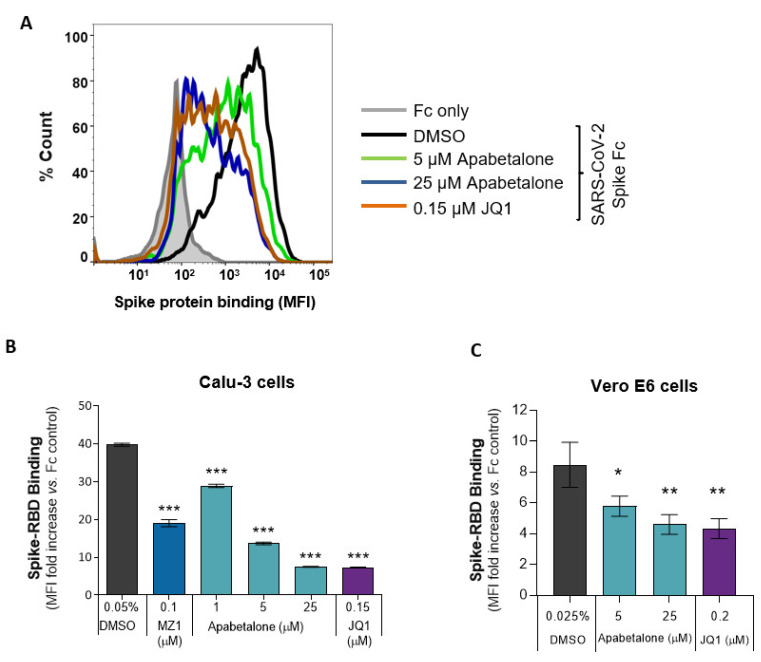
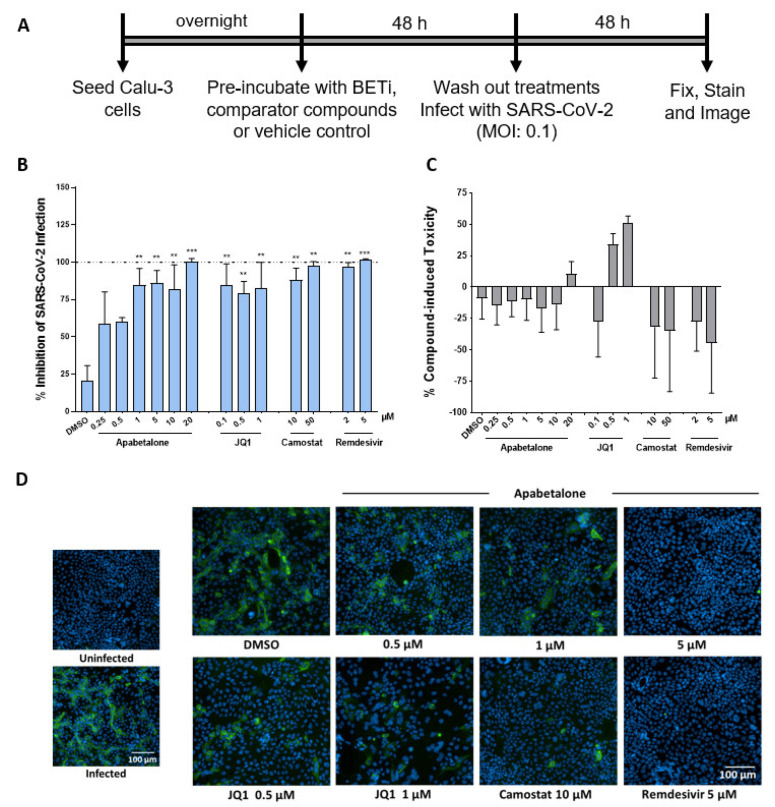
Effective therapeutics are urgently needed to counter infection and improve outcomes for patients suffering from COVID-19 and to combat this pandemic. Manipulation of epigenetic machinery to influence viral infectivity of host cells is a relatively unexplored area. The bromodomain and extraterminal (BET) family of epigenetic readers have been reported to modulate SARS-CoV-2 infection. Herein, we demonstrate apabetalone, the most clinical advanced BET inhibitor, downregulates expression of cell surface receptors involved in SARS-CoV-2 entry, including angiotensin-converting enzyme 2 (ACE2) and dipeptidyl-peptidase 4 (DPP4 or CD26) in SARS-CoV-2 permissive cells. Moreover, we show that apabetalone inhibits SARS-CoV-2 infection in vitro to levels comparable to those of antiviral agents. Taken together, our study supports further evaluation of apabetalone to treat COVID-19, either alone or in combination with emerging therapeutics.
Keywords: BET proteins; COVID-19; SARS-CoV-2; angiotensin-converting enzyme 2 (ACE2); apabetalone.
Conflict of interest statement
A.L.S., D.Y.M., A.M., S.P.M.R., and D.E.-G. have no conflicts of interest, financial or otherwise. D.G., L.F., S.C.S., J.O.J., M.S., N.C.W.W. and E.K. are employed by Resverlogix and may hold stock and/or stock options.
Figures
References
-
- The World Health Organization: Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV) [(accessed on 17 April 2021)]; Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting...
-
- Stawicki S.P., Jeanmonod R., Miller A.C., Paladino L., Gaieski D.F., Yaffee A.Q., De Wulf A., Grover J., Papadimos T.J., Bloem C., et al. The 2019–2020 novel coronavirus (severe acute respiratory syndrome coronavirus 2) pandemic: A joint american college of academic international medicine-world academic council of emergency medicine multidisciplinary COVID-19 working group consensus paper. J. Glob. Infect. Dis. 2020;12:47–93. doi: 10.4103/jgid.jgid_86_20. - DOI - PMC - PubMed
-
- Barker-Davies R.M., O’Sullivan O., Senaratne K.P.P., Baker P., Cranley M., Dharm-Datta S., Ellis H., Goodall D., Gough M., Lewis S., et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020;54:949–959. doi: 10.1136/bjsports-2020-102596. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
