

VWF, Platelets and the Antiphospholipid Syndrome
- PMID: 33919627
- PMCID: PMC8074042
- DOI: 10.3390/ijms22084200
VWF, Platelets and the Antiphospholipid Syndrome
Abstract
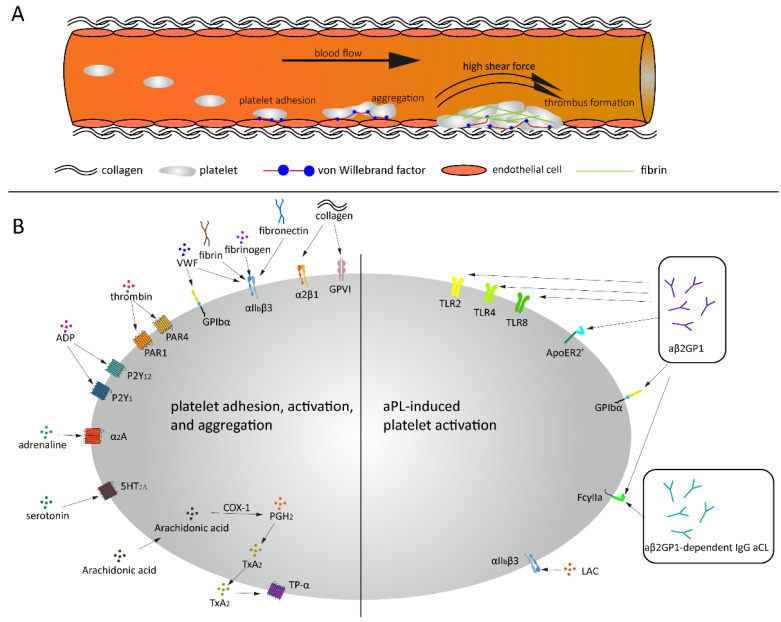
The antiphospholipid syndrome (APS) is characterized by thrombosis and/or pregnancy morbidity with the persistent presence of antiphospholipid antibodies (aPLs). Laboratory criteria for the classification of APS include the detection of lupus anticoagulant (LAC), anti-cardiolipin (aCL) antibodies and anti-β2glycoprotein I (aβ2GPI) antibodies. Clinical criteria for the classification of thrombotic APS include venous and arterial thrombosis, along with microvascular thrombosis. Several aPLs, including LAC, aβ2GPI and anti-phosphatidylserine/prothrombin antibodies (aPS/PT) have been associated with arterial thrombosis. The Von Willebrand Factor (VWF) plays an important role in arterial thrombosis by mediating platelet adhesion and aggregation. Studies have shown that aPLs antibodies present in APS patients are able to increase the risk of arterial thrombosis by upregulating the plasma levels of active VWF and by promoting platelet activation. Inflammatory reactions induced by APS may also provide a suitable condition for arterial thrombosis, mostly ischemic stroke and myocardial infarction. The presence of other cardiovascular risk factors can enhance the effect of aPLs and increase the risk for thrombosis even more. These factors should therefore be taken into account when investigating APS-related arterial thrombosis. Nevertheless, the exact mechanism by which aPLs can cause thrombosis remains to be elucidated.
Keywords: antiphospholipid antibody; antiphospholipid syndrome; arterial thrombosis; platelet; von Willebrand factor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
"Non-criteria" antiphospholipid antibodies add value to antiphospholipid syndrome diagnoses in a large Chinese cohort.Arthritis Res Ther. 2020 Feb 21;22(1):33. doi: 10.1186/s13075-020-2131-4. Arthritis Res Ther. 2020. PMID: 32085759 Free PMC article.
-
Increased platelet deposition on extracellular matrix under flow conditions in patients with antiphospholipid syndrome who experience thrombotic events.Arthritis Rheum. 2005 Dec;52(12):4011-7. doi: 10.1002/art.21437. Arthritis Rheum. 2005. PMID: 16320349
-
Diagnostic value of antibodies to phosphatidylserine/prothrombin complex for antiphospholipid syndrome in Chinese patients.Clin Rheumatol. 2017 Feb;36(2):401-406. doi: 10.1007/s10067-016-3498-0. Epub 2017 Jan 3. Clin Rheumatol. 2017. PMID: 28050648
-
Antiphospholipid Antibody-Mediated Thrombotic Mechanisms in Antiphospholipid Syndrome: Towards Pathophysiology-Based Treatment.Curr Pharm Des. 2016;22(28):4451-69. doi: 10.2174/1381612822666160527160029. Curr Pharm Des. 2016. PMID: 27229722 Review.
-
From antibody to clinical phenotype, the black box of the antiphospholipid syndrome: pathogenic mechanisms of the antiphospholipid syndrome.Thromb Res. 2013 Sep;132(3):319-26. doi: 10.1016/j.thromres.2013.07.023. Epub 2013 Aug 2. Thromb Res. 2013. PMID: 23958468 Review.
Cited by
-
Phytochemical profile and diverse pharmacology of Garcinia celebica L.Heliyon. 2024 May 3;10(9):e30629. doi: 10.1016/j.heliyon.2024.e30629. eCollection 2024 May 15. Heliyon. 2024. PMID: 38742069 Free PMC article. Review.
-
Nomogram model for identifying portal vein thrombosis in patients with decompensated cirrhosis.Eur J Gastroenterol Hepatol. 2025 Aug 1;37(8):935-942. doi: 10.1097/MEG.0000000000002968. Epub 2025 Mar 26. Eur J Gastroenterol Hepatol. 2025. PMID: 40359276 Free PMC article.
-
Antiphospholipid Antibodies Modify the Prognostic Value of Baseline Platelet Count for Clinical Outcomes After Ischemic Stroke.J Am Heart Assoc. 2024 Oct;13(19):e035183. doi: 10.1161/JAHA.124.035183. Epub 2024 Sep 30. J Am Heart Assoc. 2024. PMID: 39344638 Free PMC article.
-
An Update on Antiphospholipid Syndrome.Curr Rheumatol Rep. 2022 Jan 5;23(12):84. doi: 10.1007/s11926-021-01051-5. Curr Rheumatol Rep. 2022. PMID: 34985625 Review.
-
Synergies of Human Umbilical Vein Endothelial Cell-Laden Calcium Silicate-Activated Gelatin Methacrylate for Accelerating 3D Human Dental Pulp Stem Cell Differentiation for Endodontic Regeneration.Polymers (Basel). 2021 Sep 27;13(19):3301. doi: 10.3390/polym13193301. Polymers (Basel). 2021. PMID: 34641117 Free PMC article.
References
-
- Miyakis S., Lockshin M.D., Atsumi T., Branch D.W., Brey R.L., Cervera R., Derksen R.H., PG D.E.G., Koike T., Meroni P.L., et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J. Thromb. Haemost. 2006;4:295–306. doi: 10.1111/j.1538-7836.2006.01753.x. - DOI - PubMed
-
- van der Vorm L.N., Visser R., Huskens D., Veninga A., Adams D.L., Remijn J.A., Hemker H.C., Rensma P.L., van Horssen R., de Laat B. Circulating active von Willebrand factor levels are increased in chronic kidney disease and end-stage renal disease. Clin. Kidney J. 2020;13:72–74. doi: 10.1093/ckj/sfz076. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
