

Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial
- PMID: 33919899
- PMCID: PMC8070926
- DOI: 10.3390/healthcare9040463
Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial
Abstract
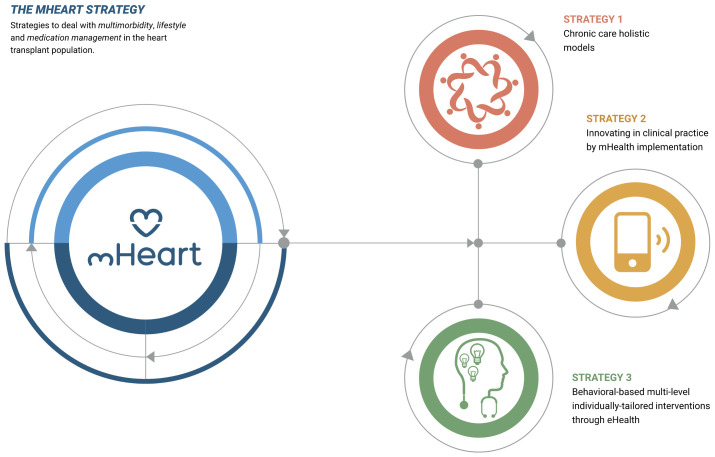
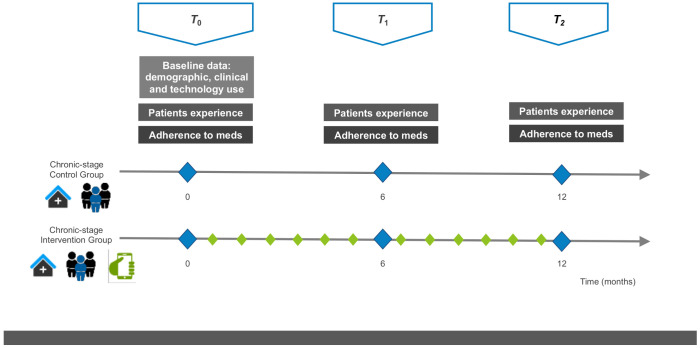
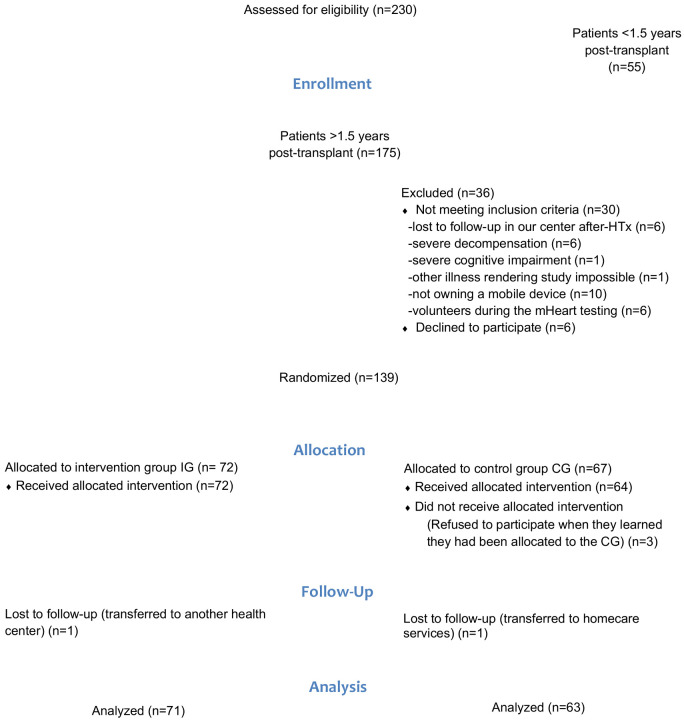
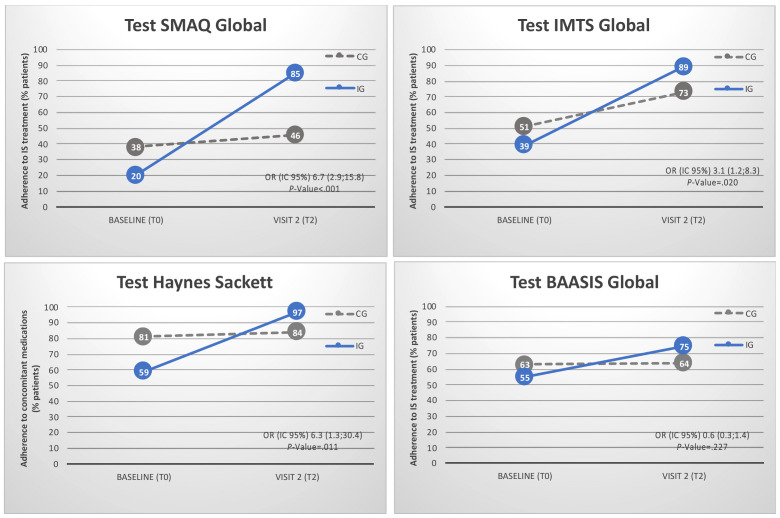
Non-adherence after heart transplantation (HTx) is a significant problem. The main objective of this study was to evaluate if a mHealth strategy is more effective than standard care in improving adherence and patients' experience in heart transplant recipients. Methods: This was a single-center, randomized controlled trial (RCT) in adult recipients >1.5 years post-HTx. Participants were randomized to standard care (control group) or to the mHeart Strategy (intervention group). For patients randomized to the mHeart strategy, multifaceted theory-based interventions were provided during the study period to optimize therapy management using the mHeart mobile application. Patient experience regarding their medication regimens were evaluated in a face-to-face interview. Medication adherence was assessed by performing self-reported questionnaires. A composite adherence score that included the SMAQ questionnaire, the coefficient of variation of drug levels and missing visits was also reported. Results: A total of 134 HTx recipients were randomized (intervention N = 71; control N = 63). Mean follow-up was 1.6 (SD 0.6) years. Improvement in adherence from baseline was significantly higher in the intervention group versus the control group according to the SMAQ questionnaire (85% vs. 46%, OR = 6.7 (2.9; 15.8), p-value < 0.001) and the composite score (51% vs. 23%, OR = 0.3 (0.1; 0.6), p-value = 0.001). Patients' experiences with their drug therapy including knowledge of their medication timing intakes (p-value = 0.019) and the drug indications or uses that they remembered (p-value = 0.003) significantly improved in the intervention versus the control group. Conclusions: In our study, the mHealth-based strategy significantly improved adherence and patient beliefs regarding their medication regimens among the HTx population. The mHeart mobile application was used as a feasible tool for providing long-term, tailor-made interventions to HTx recipients to improve the goals assessed.
Keywords: behavioral sciences; heart transplantation; immunosuppression; interdisciplinary health team; medication therapy management; mobile health; patient-reported outcome measures; telemedicine; treatment adherence and compliance; treatment outcome.
Conflict of interest statement
The mHeart® platform technology was developed by a private Spanish firm specializing in healthcare system applications (Trilema Salud S.L.). Most of the authors have collaborated as consultants. The developers had no role in the design, data collection and analysis, decision to publish, or final preparation of the studies or published manuscripts. The Hospital Research Institute owns the legal property of the mHeart national trademark and the intellectual property of the mHeart content. The authors declare no other conflicts of interest.
Figures

References
-
- Brocks Y., Zittermann A., Grisse D., Schmid-Ott G., Stock-Gießendanner S., Schulz U., Brakhage J., Benkler A., Gummert J., Tigges-Limmer K. Adherence of Heart Transplant Recipients to Prescribed Medication and Recommended Lifestyle Habits. Prog. Transpl. 2017;27:160–166. doi: 10.1177/1526924817699959. - DOI - PubMed
-
- Dew M.A., DiMartini A.F., Dabbs A.D.V., Myaskovsky L., Steel J., Unruh M., Switzer G.E., Zomak R., Kormos R.L., Greenhouse J.B. Rates and Risk Factors for Nonadherence to the Medical Regimen After Adult Solid Organ Transplantation. Transplantation. 2007;83:858–873. doi: 10.1097/01.tp.0000258599.65257.a6. - DOI - PubMed
Grants and funding
- A scientific research grant to fund the pilot study of the mHeart platform/The General Pharmaceutical Council of Barcelona
- a contribution with the Hospital to fund the technical development of the mHeart platform and the previous pilot study/Astellas Pharma SL
- A contribution with the Hospital to fund the current maintenance of the mHeart platform/Amgen SL
- Contributed to fund this clinical trial and the previous technical development of the mHeart platform/Pharmacy Department of the Hospital de la Santa Creu i Sant Pau
LinkOut - more resources
Full Text Sources
Other Literature Sources
