

Radical Resection for Locally Advanced Pancreatic Cancers in the Era of New Neoadjuvant Therapy-Arterial Resection, Arterial Divestment and Total Pancreatectomy
- PMID: 33920314
- PMCID: PMC8068970
- DOI: 10.3390/cancers13081818
Radical Resection for Locally Advanced Pancreatic Cancers in the Era of New Neoadjuvant Therapy-Arterial Resection, Arterial Divestment and Total Pancreatectomy
Abstract
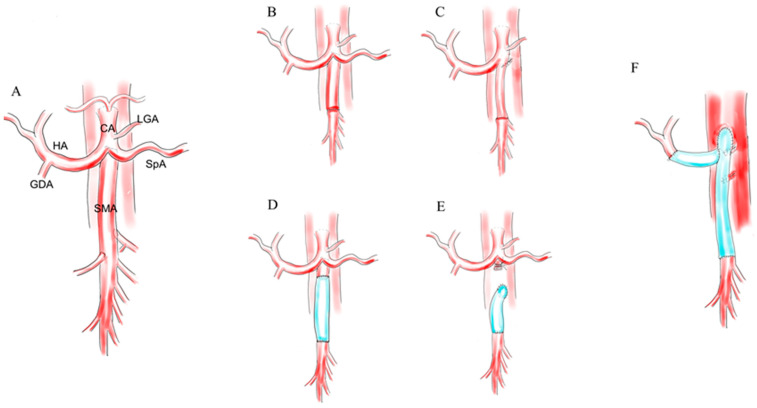
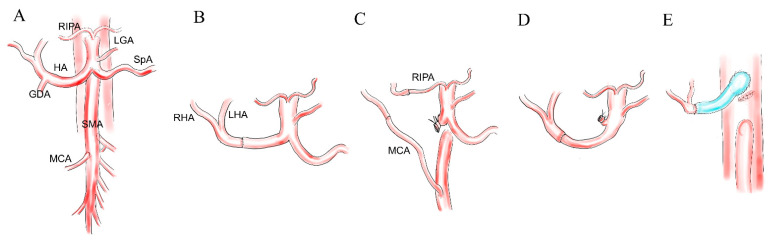
Aggressive arterial resection (AR) or total pancreatectomy (TP) in surgical treatment for locally advanced pancreatic cancer (LAPC) had long been discouraged because of their high mortality rate and unsatisfactory long-term outcomes. Recently, new chemotherapy regimens such as FOLFIRINOX or Gemcitabine and nab-paclitaxel have provided more adequate patient selection and local tumor suppression, justifying aggressive local resection. In this review, we investigate the recent reports focusing on arterial resection and total pancreatectomy for LAPC and discuss the rationale of such an aggressive approach in the treatment of PC. AR for LAPCs is divided into three, according to the target vessel. The hepatic artery resection is the simplest one, and the reconstruction methods comprise end-to-end, graft or transposition, and no reconstruction. Celiac axis resection is mainly done with distal pancreatectomy, which allows collateral arterial supply to the liver via the pancreas head. Resection of the superior mesenteric artery is increasingly reported, though its rationale is still controversial. Total pancreatectomy has been re-evaluated as an effective option to balance both the local control and postoperative safety. In conclusion, more and more aggressive pancreatectomy has become justified by the principle of total neoadjuvant therapy. Further technical standardization and optimal neoadjuvant strategy are mandatory for the global dissemination of aggressive pancreatectomies.
Keywords: arterial resection; neoadjuvant therapy; pancreatic cancer; total pancreatectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
