

Management of Synchronous Extrathoracic Oligometastatic Non-Small Cell Lung Cancer
- PMID: 33920810
- PMCID: PMC8071146
- DOI: 10.3390/cancers13081893
Management of Synchronous Extrathoracic Oligometastatic Non-Small Cell Lung Cancer
Abstract
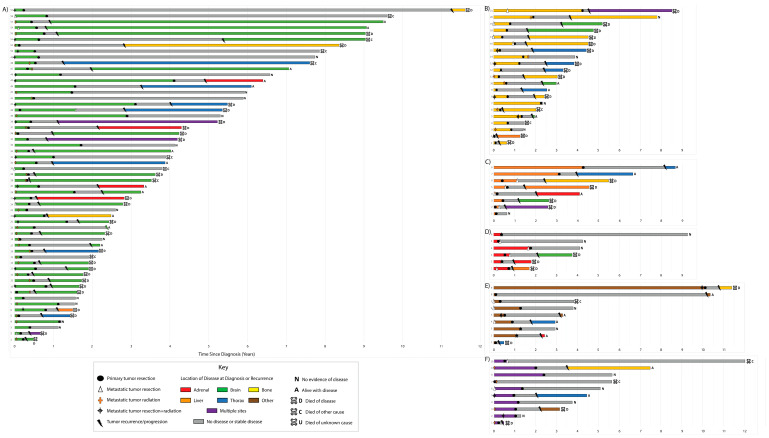
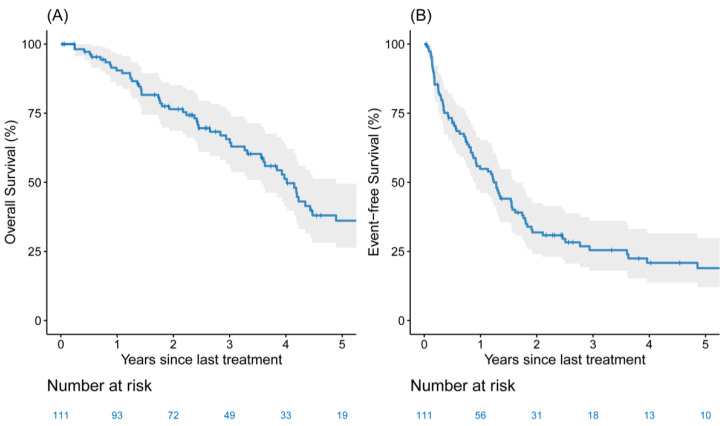
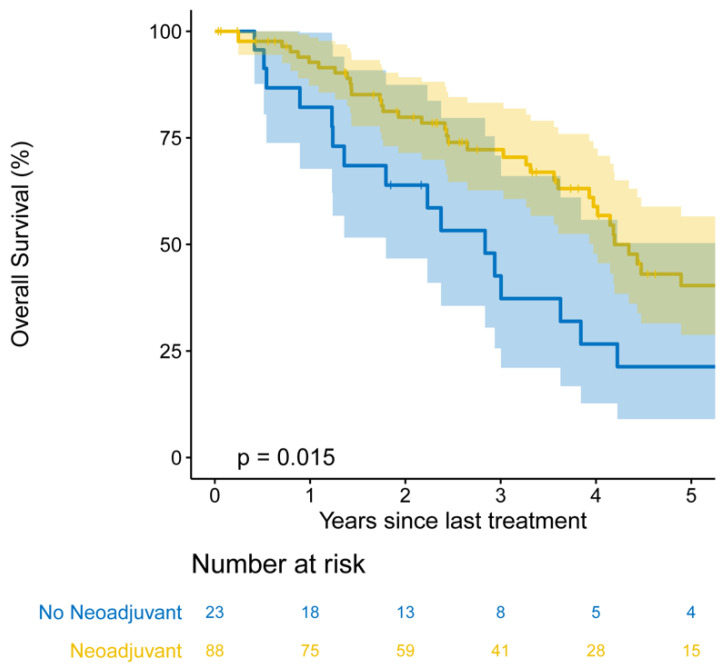
Stage IV non-small cell lung cancer (NSCLC) accounts for 35 to 40% of newly diagnosed cases of NSCLC. The oligometastatic state-≤5 extrathoracic metastatic lesions in ≤3 organs-is present in ~25% of patients with stage IV disease and is associated with markedly improved outcomes. We retrospectively identified patients with extrathoracic oligometastatic NSCLC who underwent primary tumor resection at our institution from 2000 to 2018. Event-free survival (EFS) and overall survival (OS) were estimated using the Kaplan-Meier method. Factors associated with EFS and OS were determined using Cox regression. In total, 111 patients with oligometastatic NSCLC underwent primary tumor resection; 87 (78%) had a single metastatic lesion. Local consolidative therapy for metastases was performed in 93 patients (84%). Seventy-seven patients experienced recurrence or progression. The five-year EFS was 19% (95% confidence interval (CI), 12-29%), and the five-year OS was 36% (95% CI, 27-50%). Factors independently associated with EFS were primary tumor size (hazard ratio (HR), 1.15 (95% CI, 1.03-1.29); p = 0.014) and lymphovascular invasion (HR, 1.73 (95% CI, 1.06-2.84); p = 0.029). Factors independently associated with OS were neoadjuvant therapy (HR, 0.43 (95% CI, 0.24-0.77); p = 0.004), primary tumor size (HR, 1.18 (95% CI, 1.02-1.35); p = 0.023), pathologic nodal disease (HR, 1.83 (95% CI, 1.05-3.20); p = 0.033), and visceral-pleural invasion (HR, 1.93 (95% CI, 1.10-3.40); p = 0.022). Primary tumor resection represents an important treatment option in the multimodal management of extrathoracic oligometastatic NSCLC. Encouraging long-term survival can be achieved in carefully selected patients, including those who received neoadjuvant therapy and those with limited intrathoracic disease.
Keywords: non-small cell lung cancer; oligometastasis; primary tumor resection.
Conflict of interest statement
V.W.R. reports grant support (institutional) from Genelux and Genentech, travel support from Intuitive Surgical, and travel support and payments from NIH/Coordinating Center for Clinical Trials. B.J.P. has served as a proctor for Intuitive Surgical and as a consultant for COTA. D.R.J. serves as a consultant for Merck and AstraZeneca. G.R. has financial relationships with Scanlan. All other authors have no potential conflicts to disclose.
Figures
Similar articles
-
Improved Overall Survival With Comprehensive Local Consolidative Therapy in Synchronous Oligometastatic Non-Small-Cell Lung Cancer.Clin Lung Cancer. 2020 Jan;21(1):37-46.e7. doi: 10.1016/j.cllc.2019.07.007. Epub 2019 Aug 1. Clin Lung Cancer. 2020. PMID: 31447303 Clinical Trial.
-
Long-term outcomes in radically treated synchronous vs. metachronous oligometastatic non-small-cell lung cancer.BMC Cancer. 2016 Jun 2;16:348. doi: 10.1186/s12885-016-2379-x. BMC Cancer. 2016. PMID: 27255302 Free PMC article.
-
A risk stratification scheme for synchronous oligometastatic non-small cell lung cancer developed by a multicentre analysis.Lung Cancer. 2021 Apr;154:29-35. doi: 10.1016/j.lungcan.2021.02.001. Epub 2021 Feb 12. Lung Cancer. 2021. PMID: 33610120
-
Changing equipoise in the landscape of radiation for oligometastatic lung cancer.Transl Lung Cancer Res. 2019 Sep;8(Suppl 2):S184-S191. doi: 10.21037/tlcr.2019.07.09. Transl Lung Cancer Res. 2019. PMID: 31673523 Free PMC article. Review.
-
Addition of radiotherapy to the primary tumour in oligometastatic NSCLC: A systematic review and meta-analysis.Lung Cancer. 2018 Dec;126:194-200. doi: 10.1016/j.lungcan.2018.11.017. Epub 2018 Nov 13. Lung Cancer. 2018. PMID: 30527187
Cited by
-
Exploring the Role of Preoperative Systemic Therapy and Primary Resection in NSCLC With Extrathoracic Metastases: Identifying the Optimal Candidates.Cancer Control. 2024 Jan-Dec;31:10732748241304973. doi: 10.1177/10732748241304973. Cancer Control. 2024. PMID: 39630939 Free PMC article.
-
Association between clinical outcomes and local treatment in stage IV non-small cell lung cancer patients with single extrathoracic metastasis.Thorac Cancer. 2022 May;13(9):1349-1360. doi: 10.1111/1759-7714.14398. Epub 2022 Mar 31. Thorac Cancer. 2022. PMID: 35355417 Free PMC article.
-
Benchmarking Outcomes for Molecularly Characterized Synchronous Oligometastatic Non-Small-Cell Lung Cancer Reveals EGFR Mutations to Be Associated With Longer Overall Survival.JCO Precis Oncol. 2023 Jan;7:e2200540. doi: 10.1200/PO.22.00540. JCO Precis Oncol. 2023. PMID: 36716413 Free PMC article.
-
Impact of metastasectomy on survival in patients with oligometastatic stage 4a lung cancer: a retrospective analysis.Updates Surg. 2025 Jun;77(3):937-945. doi: 10.1007/s13304-025-02120-5. Epub 2025 Feb 6. Updates Surg. 2025. PMID: 39915369 Free PMC article.
-
Evaluation of local aggressive lung therapy versus systemic therapy in oligometastatic non-small cell lung cancer: a systematic review and meta-analysis.J Thorac Dis. 2021 Oct;13(10):5899-5910. doi: 10.21037/jtd-21-957. J Thorac Dis. 2021. PMID: 34795938 Free PMC article.
References
-
- Goldstraw P., Chansky K., Crowley J., Rami-Porta R., Asamura H., Eberhardt W.E., Nicholson A.G., Groome P., Mitchell A., Bolejack V., et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016;11:39–51. doi: 10.1016/j.jtho.2015.09.009. - DOI - PubMed
-
- Dingemans A.-M.C., Hendriks L.E., Berghmans T., Levy A., Hasan B., Faivre-Finn C., Giaj-Levra M., Giaj-Levra N., Girard N., Greillier L., et al. Definition of Synchronous Oligometastatic Non–Small Cell Lung Cancer—A Consensus Report. J. Thorac. Oncol. 2019;14:2109–2119. doi: 10.1016/j.jtho.2019.07.025. - DOI - PubMed
-
- Parikh R.B., Cronin A.M., Kozono D.E., Oxnard G.R., Mak R.H., Jackman D.M., Lo P.C., Baldini E.H., Johnson B.E., Chen A.B. Definitive Primary Therapy in Patients Presenting With Oligometastatic Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. 2014;89:880–887. doi: 10.1016/j.ijrobp.2014.04.007. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
