

Myelodysplasia Syndrome, Clonal Hematopoiesis and Cardiovascular Disease
- PMID: 33921778
- PMCID: PMC8073047
- DOI: 10.3390/cancers13081968
Myelodysplasia Syndrome, Clonal Hematopoiesis and Cardiovascular Disease
Abstract
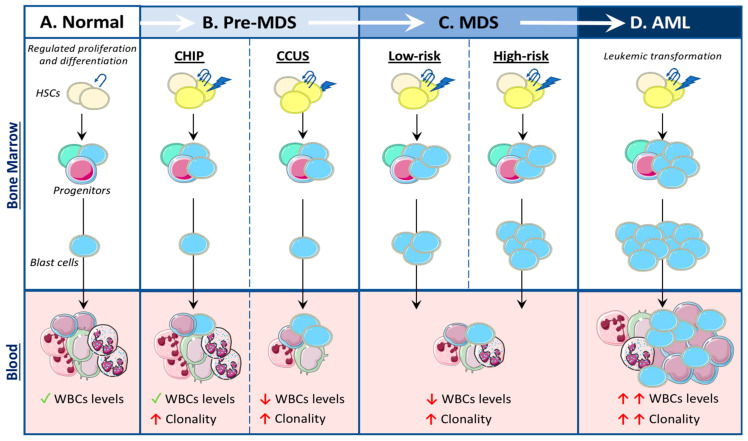
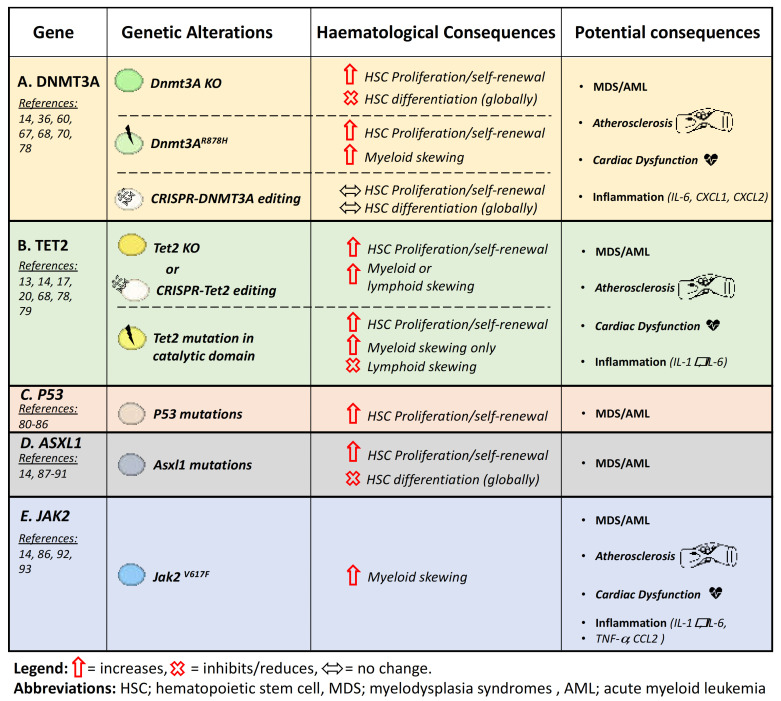
The development of myelodysplasia syndromes (MDS) is multiphasic and can be driven by a plethora of genetic mutations and/or abnormalities. MDS is characterized by a hematopoietic differentiation block, evidenced by increased immature hematopoietic cells, termed blast cells and decreased mature circulating leukocytes in at least one lineage (i.e., cytopenia). Clonal hematopoiesis of indeterminate potential (CHIP) is a recently described phenomenon preceding MDS development that is driven by somatic mutations in hemopoietic stem cells (HSCs). These mutant HSCs have a competitive advantage over healthy cells, resulting in an expansion of these clonal mutated leukocytes. In this review, we discuss the multiphasic development of MDS, the common mutations found in both MDS and CHIP, how a loss-of-function in these CHIP-related genes can alter HSC function and leukocyte development and the potential disease outcomes that can occur with dysfunctional HSCs. In particular, we discuss the novel connections between MDS development and cardiovascular disease.
Keywords: ASXL1; DNMT3A; JAK2; P53; TET2; cardiovascular disease; clonal hematopoiesis and indeterminate potential (CHIP); hematopoietic stem cell (HSC); myelodysplasia syndrome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Inflammation in myelodysplastic syndrome pathogenesis.Semin Hematol. 2024 Dec;61(6):385-396. doi: 10.1053/j.seminhematol.2024.09.005. Epub 2024 Sep 21. Semin Hematol. 2024. PMID: 39424469 Review.
-
Physician Education: Myelodysplastic Syndrome.Oncologist. 1996;1(4):284-287. Oncologist. 1996. PMID: 10388004
-
Clonal hematopoiesis: Genes and underlying mechanisms in cardiovascular disease development.J Cell Physiol. 2019 Jun;234(6):8396-8401. doi: 10.1002/jcp.27752. Epub 2018 Nov 11. J Cell Physiol. 2019. PMID: 30417440 Review.
-
Myelodysplastic syndromes are multiclonal diseases derived from hematopoietic stem and progenitor cells.Exp Hematol Oncol. 2022 May 16;11(1):28. doi: 10.1186/s40164-022-00280-3. Exp Hematol Oncol. 2022. PMID: 35578364 Free PMC article.
-
Clonal hematopoiesis: Pre-cancer PLUS.Adv Cancer Res. 2019;141:85-128. doi: 10.1016/bs.acr.2018.12.003. Epub 2019 Jan 14. Adv Cancer Res. 2019. PMID: 30691686 Review.
Cited by
-
Screening for Coronary Artery Disease in Cancer Survivors: JACC: CardioOncology State-of-the-Art Review.JACC CardioOncol. 2023 Feb 21;5(1):22-38. doi: 10.1016/j.jaccao.2022.12.007. eCollection 2023 Feb. JACC CardioOncol. 2023. PMID: 36875910 Free PMC article. Review.
-
Dynamic changes of DNA methylation induced by benzo(a)pyrene in cancer.Genes Environ. 2023 Jul 1;45(1):21. doi: 10.1186/s41021-023-00278-1. Genes Environ. 2023. PMID: 37391844 Free PMC article. Review.
-
Hematopoiesis of Indeterminate Potential and Atherothrombotic Risk.Thromb Haemost. 2022 Sep;122(9):1435-1442. doi: 10.1055/a-1830-2147. Epub 2022 Apr 20. Thromb Haemost. 2022. PMID: 35445383 Free PMC article. Review.
-
CHIP-associated mutant ASXL1 in blood cells promotes solid tumor progression.Cancer Sci. 2022 Apr;113(4):1182-1194. doi: 10.1111/cas.15294. Epub 2022 Feb 26. Cancer Sci. 2022. PMID: 35133065 Free PMC article.
-
Rare-variant collapsing analyses of arterial hypertension in the UK biobank.J Hum Hypertens. 2023 Nov;37(11):1040-1042. doi: 10.1038/s41371-023-00829-7. Epub 2023 Apr 14. J Hum Hypertens. 2023. PMID: 37059828 Free PMC article. No abstract available.
References
-
- Arber D.A., Orazi A., Hasserjian R., Thiele J., Borowitz M.J., Le Beau M.M., Bloomfield C.D., Cazzola M., Vardiman J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–2405. doi: 10.1182/blood-2016-03-643544. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
