

A Non-Linear Biostatistical Graphical Modeling of Preventive Actions and Healthcare Factors in Controlling COVID-19 Pandemic
- PMID: 33922634
- PMCID: PMC8122857
- DOI: 10.3390/ijerph18094491
A Non-Linear Biostatistical Graphical Modeling of Preventive Actions and Healthcare Factors in Controlling COVID-19 Pandemic
Abstract
Background: With the insurgence of the COVID-19 pandemic, many people died in the past several months, and the situation is ongoing with increasing health, social, and economic panic and vulnerability. As most of the countries relying on different preventive actions to control the outcomes of COVID-19, it is necessary to boost the knowledge about the effectiveness of such actions so that the policymakers take their country-based appropriate actions. This study generates evidence of taking the most impactful actions to combat COVID-19.
Objective: In order to generate community-based scientific evidence, this study analyzed the outcome of COVID-19 in response to different control measures, healthcare facilities, life expectancy, and prevalent diseases.
Methods: It used more than a hundred countries' data collected from different databases. We performed a comparative graphical analysis with non-linear correlation estimation using R.
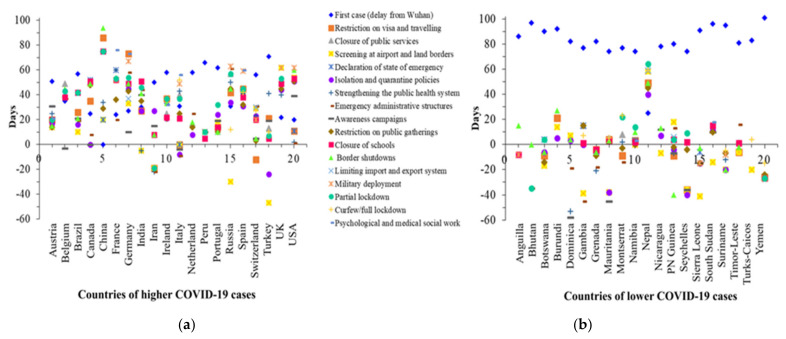
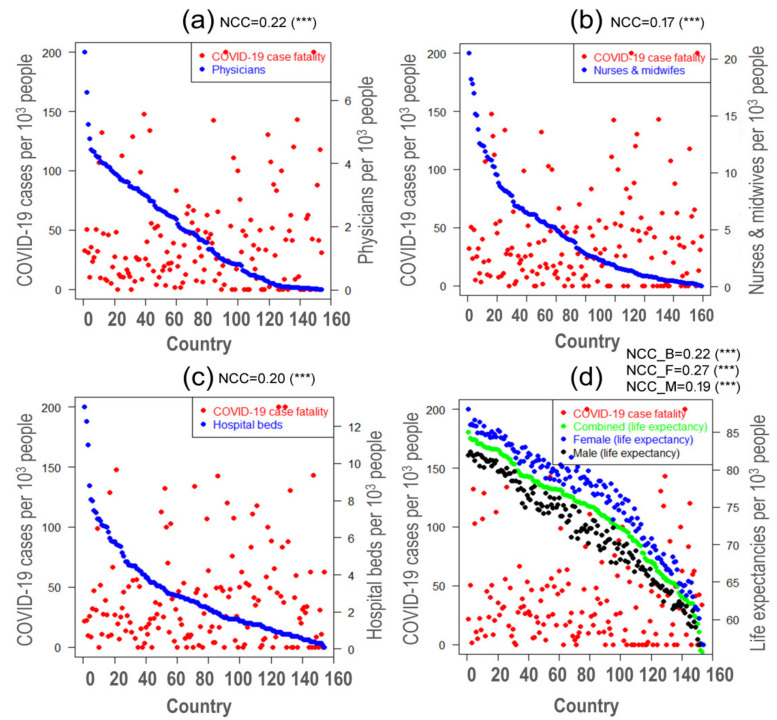
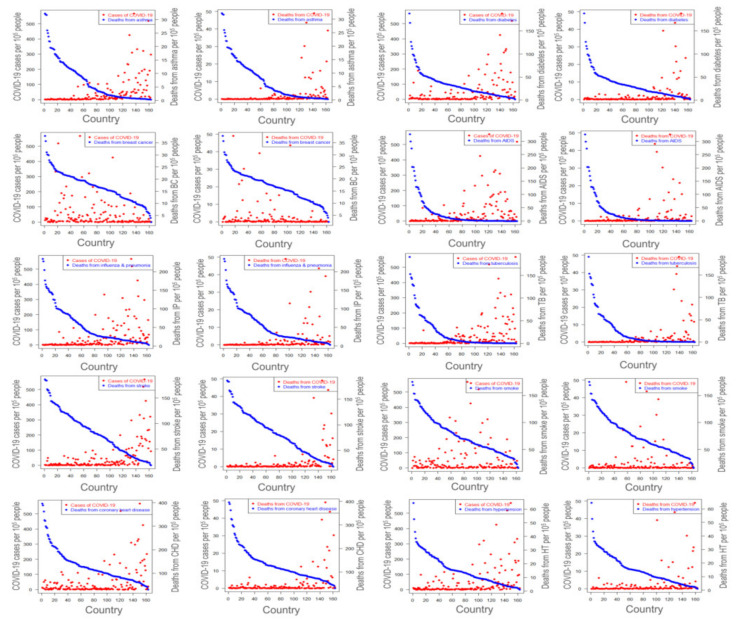
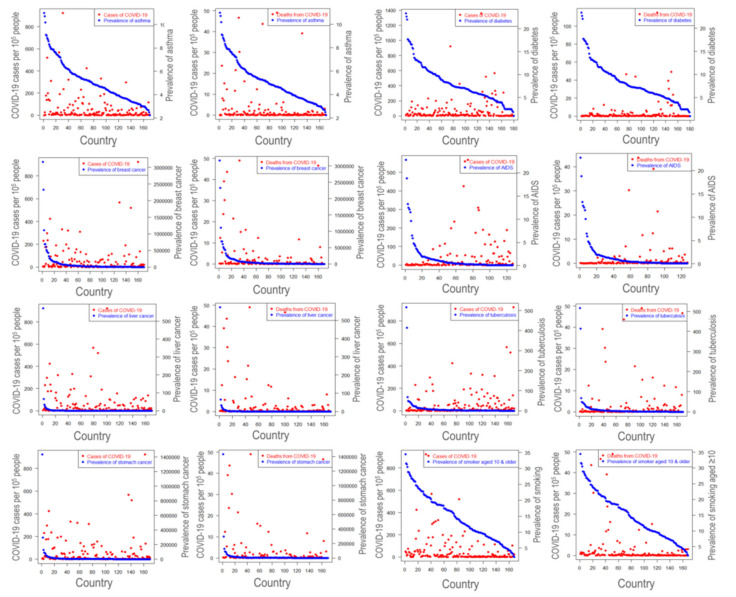
Results: The reduction of COVID-19 cases is strongly correlated with the earliness of preventive initiation. The apathy of taking nationwide immediate precaution measures has been identified as one of the critical reasons to make the circumstances worse. There is significant non-linear relationship between COVID-19 case fatality and number of physicians (NCC = 0.22; p-value ≤ 0.001), nurses and midwives (NCC = 0.17; p-value ≤ 0.001), hospital beds (NCC = 0.20; p-value ≤ 0.001), life expectancy of both sexes (NCC = 0.22; p-value ≤ 0.001), life expectancy of female (NCC = 0.27; p-value ≤ 0.001), and life expectancy of male (NCC = 0.19; p-value ≤ 0.001). COVID-19 deaths were found to be reduced with increased medical personnel and hospital beds. Interestingly, no association between the comorbidities and severity of COVID-19 was found excluding asthma, cancer, Alzheimer's, and smoking.
Conclusions: Enhancing healthcare facilities and early imposing the control measures could be valuable to prevent the COVID-19 pandemic. No association between COVID-19 and other comorbidities warranted further investigation at the pathobiological level.
Keywords: COVID-19 pandemic; case fatality rate; life expectancy; lockdown; quarantine; social distance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Travel-related control measures to contain the COVID-19 pandemic: a rapid review.Cochrane Database Syst Rev. 2020 Oct 5;10:CD013717. doi: 10.1002/14651858.CD013717. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 25;3:CD013717. doi: 10.1002/14651858.CD013717.pub2. PMID: 33502002 Updated.
-
[Mental health care in French correctional facilities during the Covid-19 pandemic].Encephale. 2020 Jun;46(3S):S60-S65. doi: 10.1016/j.encep.2020.05.002. Epub 2020 May 8. Encephale. 2020. PMID: 32475693 Free PMC article. French.
-
SARS-CoV-2 pandemic and Construction Industry: insights from Italian data.Acta Biomed. 2022 Jul 1;93(3):e2022233. doi: 10.23750/abm.v93i3.12265. Acta Biomed. 2022. PMID: 35775779 Free PMC article.
-
The impact of government pandemic policies on the vulnerability of healthcare workers to SARS-CoV-2 infection and mortality in Jakarta Province, Indonesia.Ann Med. 2023;55(2):2293306. doi: 10.1080/07853890.2023.2293306. Epub 2024 Jan 11. Ann Med. 2023. PMID: 38206905 Free PMC article.
-
International travel-related control measures to contain the COVID-19 pandemic: a rapid review.Cochrane Database Syst Rev. 2021 Mar 25;3(3):CD013717. doi: 10.1002/14651858.CD013717.pub2. Cochrane Database Syst Rev. 2021. PMID: 33763851 Free PMC article.
Cited by
-
Effect of total population, population density and weighted population density on the spread of Covid-19 in Malaysia.PLoS One. 2023 Apr 27;18(4):e0284157. doi: 10.1371/journal.pone.0284157. eCollection 2023. PLoS One. 2023. PMID: 37104371 Free PMC article.
-
Modelling COVID-19 pandemic control strategies in metropolitan and rural health districts in New South Wales, Australia.Sci Rep. 2023 Jun 26;13(1):10352. doi: 10.1038/s41598-023-37240-8. Sci Rep. 2023. PMID: 37365205 Free PMC article.
-
A Review of COVID-19 Modelling Strategies in Three Countries to Develop a Research Framework for Regional Areas.Viruses. 2021 Oct 29;13(11):2185. doi: 10.3390/v13112185. Viruses. 2021. PMID: 34834990 Free PMC article. Review.
-
Burden of COVID-19 on health and wellbeing, education, and economy of Bangladesh.Clin Case Rep. 2022 Nov 23;10(11):e6639. doi: 10.1002/ccr3.6639. eCollection 2022 Nov. Clin Case Rep. 2022. PMID: 36439388 Free PMC article.
-
Factors influencing plasma donation behavior of COVID-19 recovered patients in Bangladesh: A pilot study.Health Sci Rep. 2022 Dec 2;6(1):e974. doi: 10.1002/hsr2.974. eCollection 2023 Jan. Health Sci Rep. 2022. PMID: 36479388 Free PMC article.
References
-
- Gorbalenya A.E., Baker S.C., Baric R.S., de Groot R.J., Drosten C., Gulyaeva A.A., Haagmans B.L., Lauber C., Leontovich A.M., Neuman B.W., et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020;5:536–544. doi: 10.1038/s41564-020-0695-z. - DOI - PMC - PubMed
-
- Hasanul M., Siam B., Md S., Abedin M., Ahmed A., Nishat N.H., Hossain M.S., Rahman M.M. Pathophysiological mechanisms of disease severity in COVID-19: An update. J. Adv. Biotechnol. Exp. Ther. 2020;3:68–77. doi: 10.5455/jabet.2020.d158. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
