

Current State of Analgesia and Sedation in the Pediatric Intensive Care Unit
- PMID: 33922824
- PMCID: PMC8122992
- DOI: 10.3390/jcm10091847
Current State of Analgesia and Sedation in the Pediatric Intensive Care Unit
Abstract
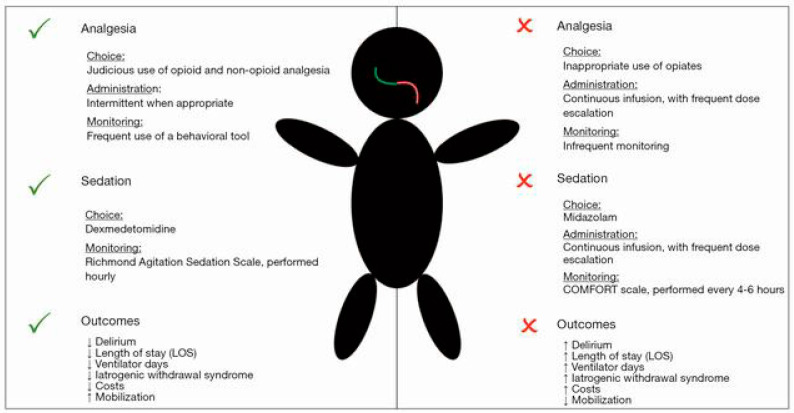
Critically ill pediatric patients often require complex medical procedures as well as invasive testing and monitoring which tend to be painful and anxiety-provoking, necessitating the provision of analgesia and sedation to reduce stress response. Achieving the optimal combination of adequate analgesia and appropriate sedation can be quite challenging in a patient population with a wide spectrum of ages, sizes, and developmental stages. The added complexities of critical illness in the pediatric population such as evolving pathophysiology, impaired organ function, as well as altered pharmacodynamics and pharmacokinetics must be considered. Undersedation leaves patients at risk of physical and psychological stress which may have significant long term consequences. Oversedation, on the other hand, leaves the patient at risk of needing prolonged respiratory, specifically mechanical ventilator, support, prolonged ICU stay and hospital admission, and higher risk of untoward effects of analgosedative agents. Both undersedation and oversedation put critically ill pediatric patients at high risk of developing PICU-acquired complications (PACs) like delirium, withdrawal syndrome, neuromuscular atrophy and weakness, post-traumatic stress disorder, and poor rehabilitation. Optimal analgesia and sedation is dependent on continuous patient assessment with appropriately validated tools that help guide the titration of analgosedative agents to effect. Bundled interventions that emphasize minimizing benzodiazepines, screening for delirium frequently, avoiding physical and chemical restraints thereby allowing for greater mobility, and promoting adequate and proper sleep will disrupt the PICU culture of immobility and reduce the incidence of PACs.
Keywords: PICU; PICU-acquired complications; analgesia; critically ill pediatric patient; delirium; sedation; withdrawal.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Choong K. PICU-acquired complications: The new marker of the quality of care. ICU Manag. Pract. 2019;19:85–88.
-
- Doha N., El-Henawy T., Mohammed M. Analgesia and sedation for patients in the intensive care unit: A systematic review. Menoufia Med. J. 2020;33:339–345. doi: 10.4103/mmj.mmj_417_18. - DOI
-
- Curley M.A., Wypij D., Watson R.S., Grant M.J., Asaro L.A., Cheifetz I.M., Dodson B.L., Franck L.S., Gedeit R.G., Angus D.C., et al. Protocolized sedation vs. usual care in pediatric patients mechanically ventilated for acute respiratory failure: A randomized clinical trial. JAMA. 2015;313:379–389. doi: 10.1001/jama.2014.18399. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
