

Evaluation of Correlations between Genetic Variants and High-Resolution Computed Tomography Patterns in Idiopathic Pulmonary Fibrosis
- PMID: 33922858
- PMCID: PMC8146750
- DOI: 10.3390/diagnostics11050762
Evaluation of Correlations between Genetic Variants and High-Resolution Computed Tomography Patterns in Idiopathic Pulmonary Fibrosis
Abstract
Background: Idiopathic pulmonary fibrosis (IPF) is a progressive fibrosing interstitial lung disease (ILD). This prospective observational study aimed at the evaluation of any correlation between genetic variants associated with IPF susceptibility and high-resolution computed tomography (HRCT) patterns. It also aimed at evidencing any differences in the HRTC pattern between the familial and sporadic form at diagnosis and after two years.
Methods: A total of 65 IPF patients (mean age at diagnosis 65 ± 10) were enrolled after having given written informed consent. HRCT and genetic evaluations were performed.
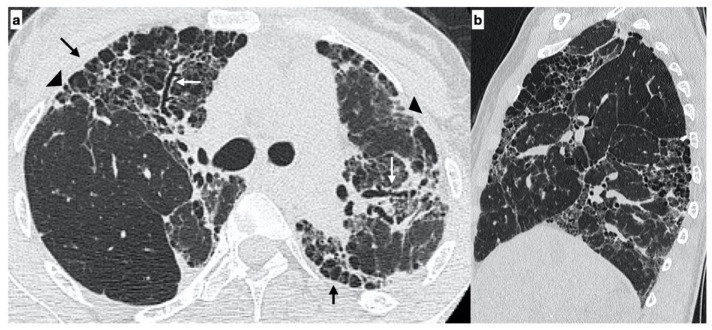
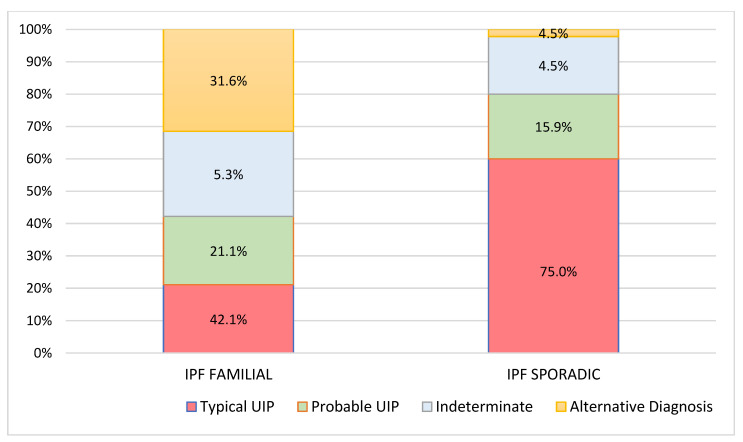
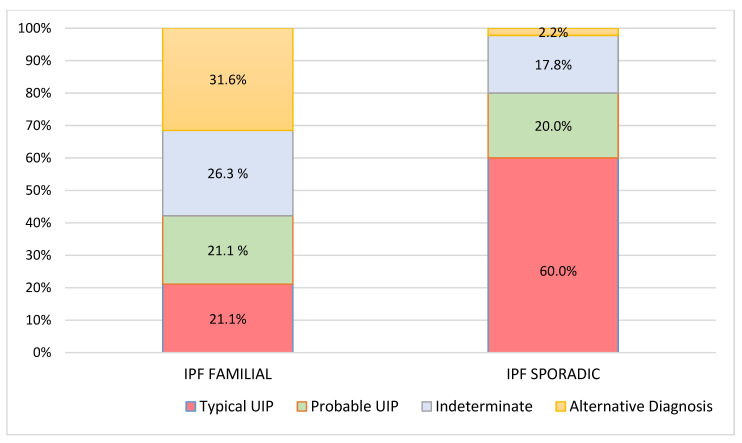
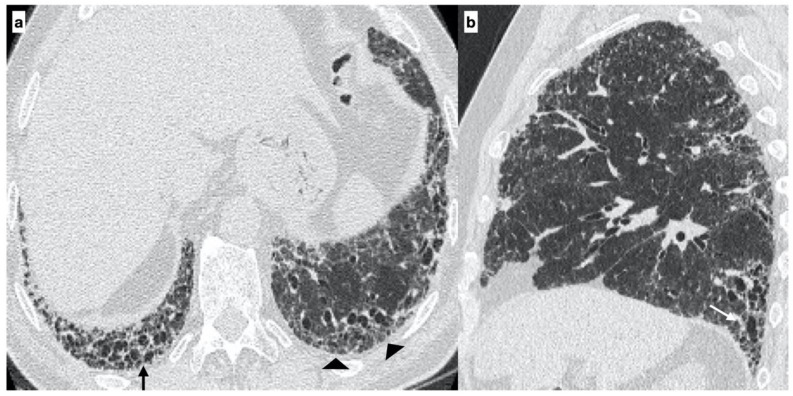
Results: A total of 19 familial (mean age 62 ± 15) and 46 sporadic (mean age 70 ± 9) IPF patients were enrolled. A statistically significant difference was evidenced in the HRTC pattern at diagnosis between the two groups. Sporadic IPF patients had a predominantly usual interstitial pneumonia (UIP) pattern compared with those patients with familial IPF (60.0% vs. 21.1%, respectively). Moreover, familial IPF patients had more alternative diagnoses than those with sporadic IPF (31.6% vs. 2.2%, respectively). Furthermore, there was a slight increase in the typical UIP pattern in the familial IPF group at two years from diagnosis.
Conclusions: Genetic factors play a pivotal role in the risk of developing IPF. However, further studies are required to clarify how these genetic factors may guide clinical treatment decisions.
Keywords: familial idiopathic pulmonary fibrosis; high-resolution computed tomography (HRCT); idiopathic pulmonary fibrosis; interstitial lung disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Raghu G., Remy-Jardin M., Myers J.L., Richeldi L., Ryerson C.J., Lederer D.J., Behr J., Cottin V., Danoff S.K., Morell F., et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018;198:e44–e68. doi: 10.1164/rccm.201807-1255ST. - DOI - PubMed
LinkOut - more resources
Full Text Sources
