

Modeling Hepatocellular Carcinoma Cells Dynamics by Serological and Imaging Biomarkers to Explain the Different Responses to Sorafenib and Regorafenib
- PMID: 33922938
- PMCID: PMC8123288
- DOI: 10.3390/cancers13092064
Modeling Hepatocellular Carcinoma Cells Dynamics by Serological and Imaging Biomarkers to Explain the Different Responses to Sorafenib and Regorafenib
Abstract
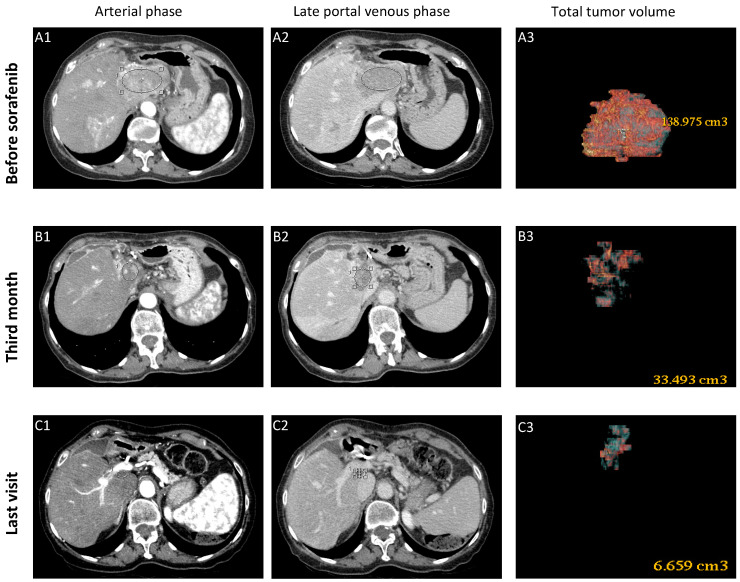
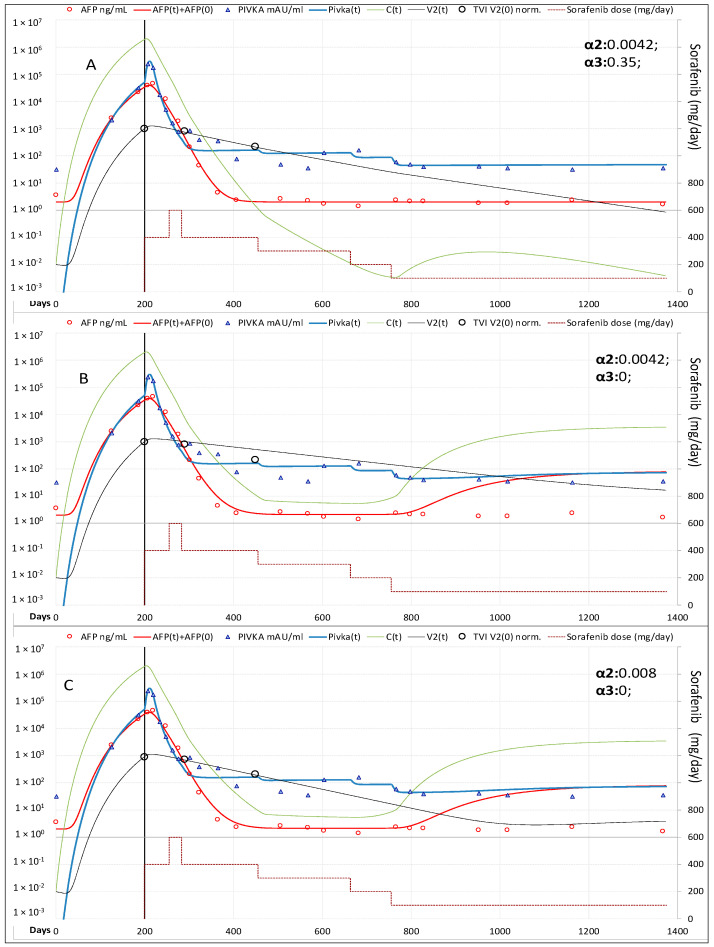
In advanced HCC, tyrosine-kinase inhibitors obtain partial responses (PR) in some patients and complete responses (CR) in a few. Better understanding of the mechanism of response could be achieved by the radiomic approach combining digital imaging and serological biomarkers (α-fetoprotein, AFP and protein induced by vitamin K absence-II, PIVKA-II) kinetics. A physic-mathematical model was developed to investigate cancer cells and vasculature dynamics in three prototype patients receiving sorafenib and/or regorafenib and applied in seven others for validation. Overall four patients showed CR, two PR, two stable-disease (SD) and two progressive-disease (PD). The rate constant of cancer cells production was higher in PD than in PR-SD and CR (median: 0.398 vs. 0.325 vs. 0.316 C × day-1). Therapy induced reduction of neo-angiogenesis was greater in CR than in PR-SD and PD (median: 83.2% vs. 29.4% and 2.0%), as the reduction of cell-proliferation (55.2% vs. 7.6% and 0.7%). An additional dose-dependent acceleration of tumor vasculature decay was also observed in CR. AFP and cancer cells followed the same kinetics, whereas PIVKA-II time/dose dependent fluctuations were influenced also by tissue ischemia. In conclusion, pending confirmation in a larger HCC cohort, modeling serological and imaging biomarkers could be a new tool for systemic therapy personalization.
Keywords: AFP; HCC; PIVKA-II; digital imaging; hepatocellular carcinoma; kinetics; mathematical modeling; regorafenib; sorafenib.
Conflict of interest statement
P.C. has served as an advisory board member for Intercept, Gilead and AbbVie, F.B. has served as a speaker for Gilead and Roche; M.R.B. has served as a speaker for AbbVie, Eisai, Gilead, Janssen, MSD and as an advisory board member for Abbott, AbbVie, Gilead, Janssen, Roche and Biotest. All other authors have no conflicts of interest to declare. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures







References
-
- GLOBOCAN 2018 The Global Cancer Observatory. International Agency for Research on Cancer 2020. [(accessed on 30 December 2020)]; Available online: http://gco.iarc.fr/today/online-analysis-table.
-
- Campigotto M., Giuffrè M., Colombo A., Visintin A., Aversano A., Budel M., Masutti F., Abazia C., Crocé L.S. Comparison between hepatocellular carcinoma prognostic scores: A 10-year single-center experience and brief review of the current literature. WJH. 2020;12:1239–1257. doi: 10.4254/wjh.v12.i12.1239. - DOI - PMC - PubMed
-
- Wilhelm S.M., Carter C., Tang L., Wilkie D., McNabola A., Rong H., Chen C., Zhang X., Vincent P., McHugh M., et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64:7099–7109. doi: 10.1158/0008-5472.CAN-04-1443. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
