

Induction of Apoptosis, Inhibition of MCL-1, and VEGF-A Expression Are Associated with the Anti-Cancer Efficacy of Magnolol Combined with Regorafenib in Hepatocellular Carcinoma
- PMID: 33922992
- PMCID: PMC8123296
- DOI: 10.3390/cancers13092066
Induction of Apoptosis, Inhibition of MCL-1, and VEGF-A Expression Are Associated with the Anti-Cancer Efficacy of Magnolol Combined with Regorafenib in Hepatocellular Carcinoma
Abstract
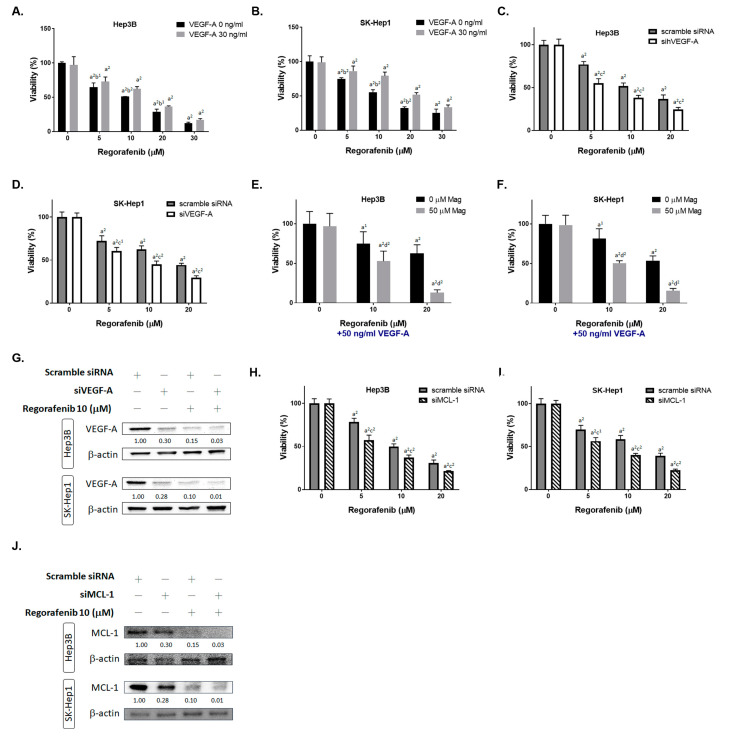
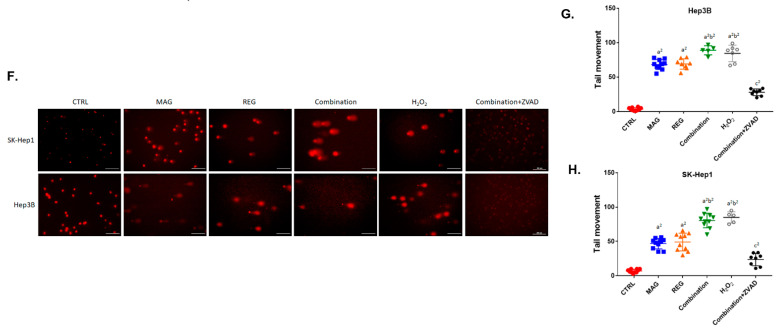
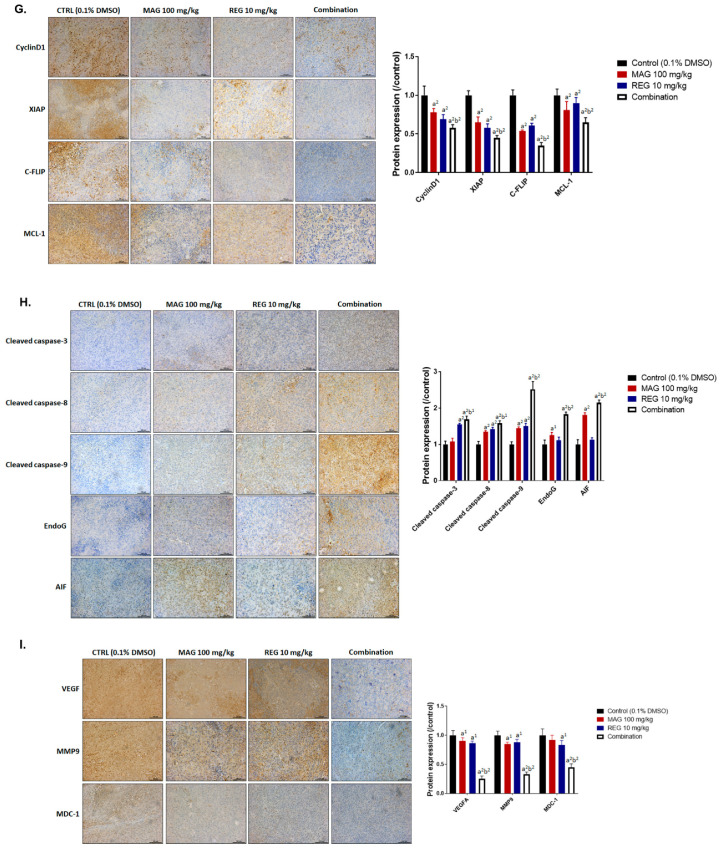
While regorafenib was approved for the treatment of advanced HCC in 2017, with a partial response and survival benefit; other combination agents to facilitate the efficacy of regorafenib still need to be explored. Magnolol is a potential natural anti-tumor compound for many types of cancers. Combination indexes calculated on the basis of both in vitro and in vivo models have indicated a synergistic effect of the combination of regorafenib and magnolol. The overexpression of the VEGF-A protein significantly diminished regorafenib's inhibition of cell viability, while the transient knockdown of VEGF-A by siRNA effectively sensitized HCC cells to regorafenib. In addition, the inhibition of MCL-1 by siRNA combined with regorafenib allowed for a significantly greater inhibition of cell growth, compared to regorafenib alone. A lower protein expression level for VEGF-A and MCL-1 was found for the combination treatment of HCC in vitro and in vivo. A superior metastasis inhibition was also found in the combination group, as compared to the single-treatment groups, using a transwell assay, wound healing assay, and Western blotting. The caspase-dependent and -independent and DNA damage effects, as determined by flow cytometry and a comet assay, were increased by the combination therapy. Taken together, magnolol sensitized HCC to regorafenib, which was correlated with the reduction of VEGF-A and MCL-1 and the induction of apoptosis.
Keywords: MCL-1; VEGF-A; apoptosis; hepatocellular carcinoma; magnolol; regorafenib.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- D’Alessandro R., Refolo M.G., Iacovazzi P.A., Pesole P.L., Messa C., Carr B.I. Ramucirumab and GSK1838705A Enhance the Inhibitory Effects of Low Concentration Sorafenib and Regorafenib Combination on HCC Cell Growth and Motility. Cancers. 2019;11:787. doi: 10.3390/cancers11060787. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
