

Overview of Non-Alcoholic Fatty Liver Disease (NAFLD) and the Role of Sugary Food Consumption and Other Dietary Components in Its Development
- PMID: 33923255
- PMCID: PMC8145877
- DOI: 10.3390/nu13051442
Overview of Non-Alcoholic Fatty Liver Disease (NAFLD) and the Role of Sugary Food Consumption and Other Dietary Components in Its Development
Abstract
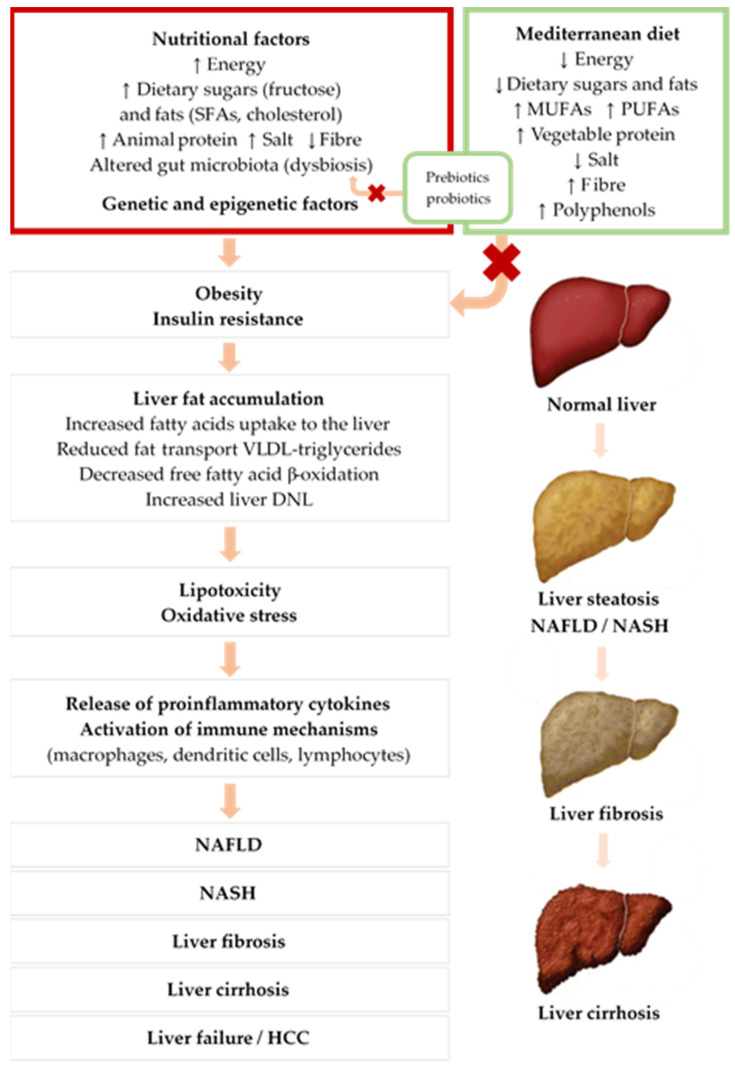
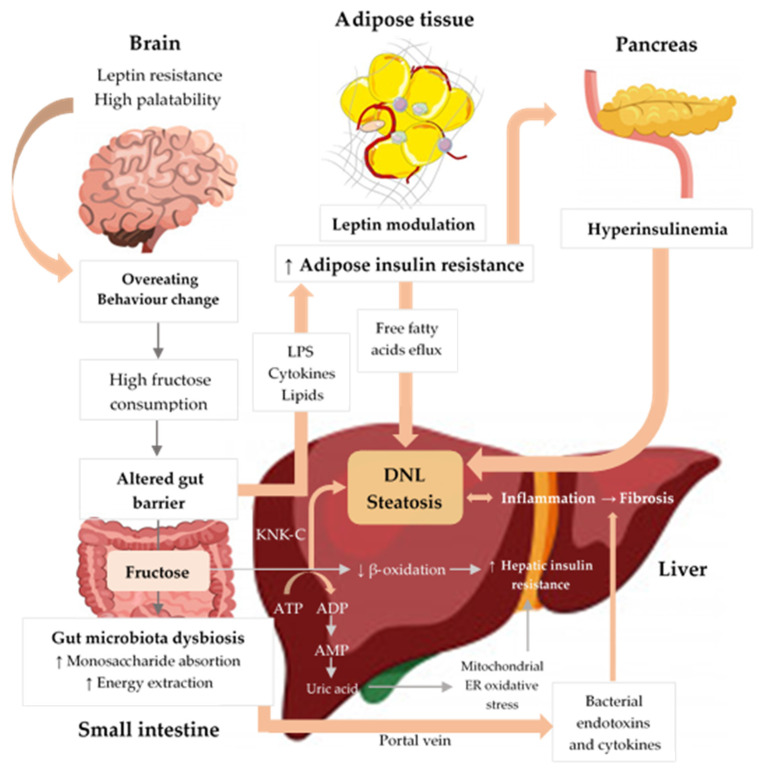
NAFLD is the world's most common chronic liver disease, and its increasing prevalence parallels the global rise in diabetes and obesity. It is characterised by fat accumulation in the liver evolving to non-alcoholic steatohepatitis (NASH), an inflammatory subtype that can lead to liver fibrosis and cirrhosis. Currently, there is no effective pharmacotherapeutic treatment for NAFLD. Treatment is therefore based on lifestyle modifications including changes to diet and exercise, although it is unclear what the most effective form of intervention is. The aim of this review, then, is to discuss the role of specific nutrients and the effects of different dietary interventions on NAFLD. It is well established that an unhealthy diet rich in calories, sugars, and saturated fats and low in polyunsaturated fatty acids, fibre, and micronutrients plays a critical role in the development and progression of this disease. However, few clinical trials have evaluated the effects of nutrition interventions on NAFLD. We, therefore, summarise what is currently known about the effects of macronutrients, foods, and dietary patterns on NAFLD prevention and treatment. Most current guidelines recommend low-calorie, plant-based diets, such as the Mediterranean diet, as the most effective dietary pattern to treat NAFLD. More clinical trials are required, however, to identify the best evidence-based dietary treatment approach.
Keywords: Mediterranean diet; NAFLD; NASH; cardiovascular disease; diabetes; fatty acids; fructose; metabolic syndrome; nutrition; protein.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Estes C., Anstee Q.M., Arias-Loste M.T., Bantel H., Bellentani S., Caballeria J., Colombo M., Craxi A., Crespo J., Day C.P., et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 2018;69:896–904. doi: 10.1016/j.jhep.2018.05.036. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
