

Molecular Mechanisms of Atopic Dermatitis Pathogenesis
- PMID: 33923629
- PMCID: PMC8074061
- DOI: 10.3390/ijms22084130
Molecular Mechanisms of Atopic Dermatitis Pathogenesis
Abstract
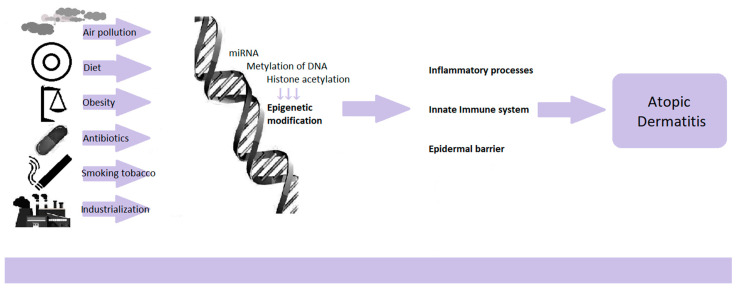
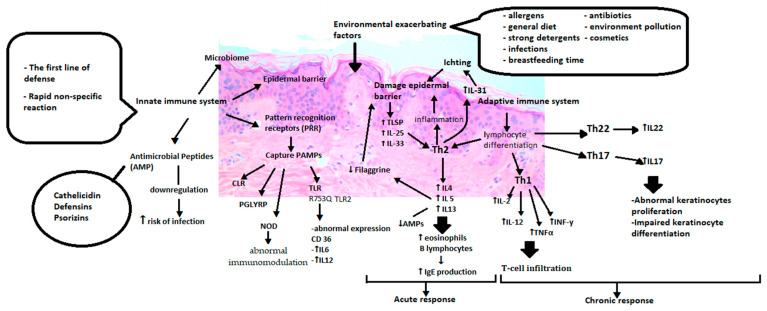
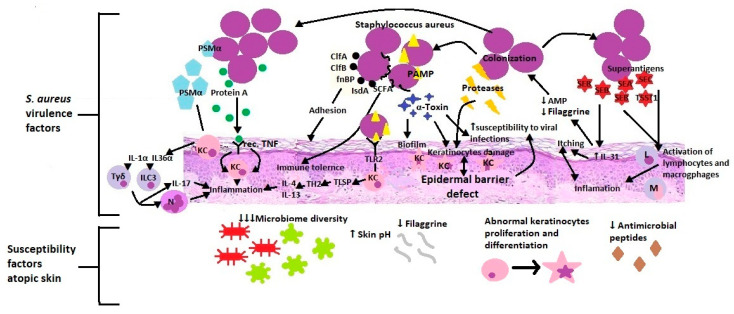
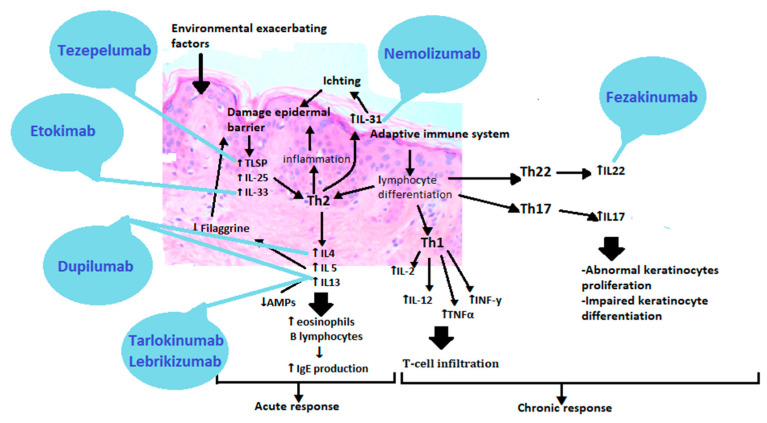
Atopic dermatitis is a chronic, non-infectious inflammatory dermatosis. Acharacteristic feature is persistent itching of the skin. The chronic, relapsing course of the disease, economic burden, and the whole family's involvement in the treatment process immensely reduce the quality of life of patients and their families. The disease emerges as a social problem by increasing indirect costs, such as visiting a doctor, absenteeism from work and school, and avoiding social interactions. Thepathophysiology of atopic dermatitis is complex and multifactorial. It includes genetic disorders, a defect in the epidermal barrier, an altered immune response, anddisruption of the skin's microbial balance. The numerous complex changes at thegenetic level and innate and adaptive immunity provide the basis for characterizing the various phenotypes and endotypes of atopic dermatitis. Emerging therapies rely on the action of specific molecules involved in the disease's pathogenesis. It may be the starting point for the individualization of atopic dermatitis treatment. This paper will try to present some molecular mechanisms of atopic dermatitis and their clinical implications.
Keywords: allergic diseases; atopic dermatitis; epidermal barriers defects; genetic disorders; immunological disturbances; microbiome; pathogenesis; targeted therapies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Asher M.I., Montefort S., Björkstén B., Lai C.K., Strachan D.P., Weiland S.K., Williams H., ISAAC Phase Three Study Group Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368:733–743. doi: 10.1016/S0140-6736(06)69283-0. - DOI - PubMed
-
- Avena-Woods C. Overview of atopic dermatitis. Am. J. Manag. Care. 2017;23(Suppl. 8):S115–S123. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
