

Iatrogenic Ocular Surface Diseases Occurring during and/or after Different Treatments for Ocular Tumours
- PMID: 33923737
- PMCID: PMC8073875
- DOI: 10.3390/cancers13081933
Iatrogenic Ocular Surface Diseases Occurring during and/or after Different Treatments for Ocular Tumours
Abstract
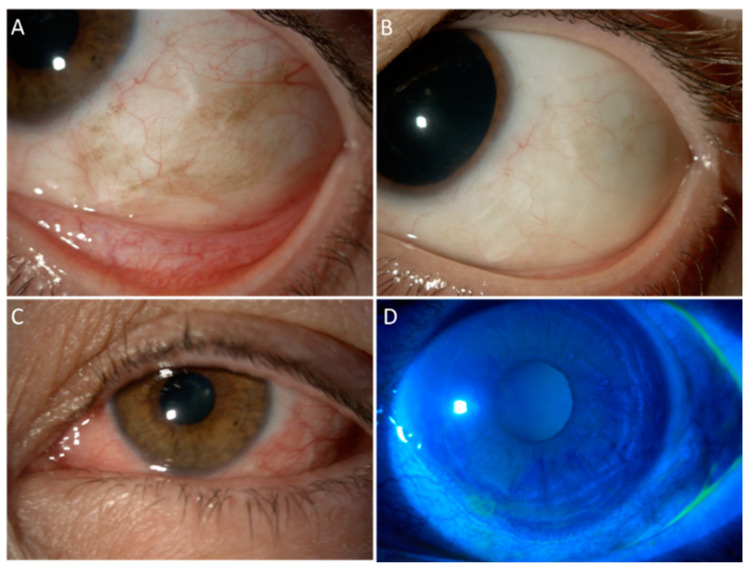
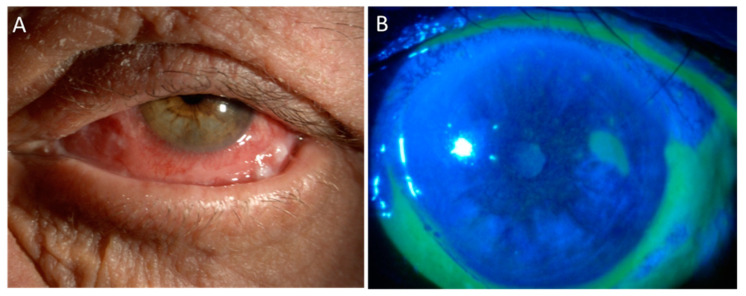
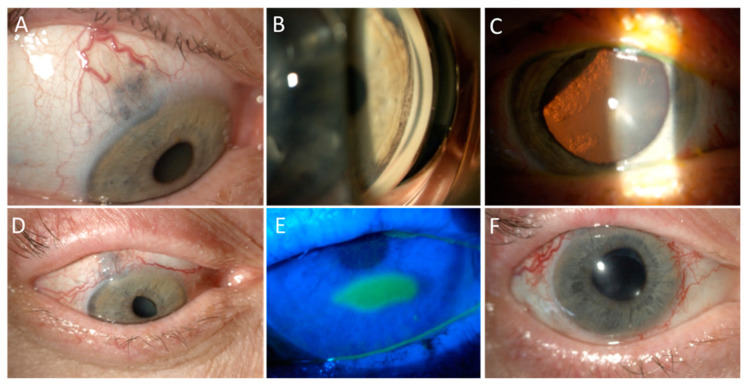
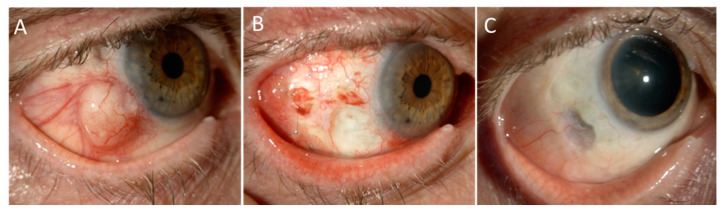
The ocular surface represents a finely regulated system that allows the protection of the eye. It is particularly susceptible to different treatments for intraocular tumours, such as uveal melanoma and conjunctival cancers. Traditionally, the management of ocular tumours depends on the characteristics of the lesion, and is based on a combination of selective surgery, topical chemotherapy, and/or radiotherapy delivered through different mechanisms (e.g., charged-particle radiotherapy or brachytherapy). Possible complications involving the ocular surface range from transient dry eye disease or keratitis up to corneal melting and perforation, which in any case deserve careful evaluation for the risk of permanent sigh-threatening complications. Clinicians involved in the management of these patients must be aware of this risk, in order to reach an early diagnosis and promptly set up an adequate treatment. The present review of the literature will summarize acute and chronic complications affecting the ocular surface following different therapies for the treatment of ocular tumours.
Keywords: anti-cancer agents; choroidal melanoma; complications; dry eye; ocular surface; ocular surface squamous neoplasia; ocular tumours; radiotherapy; uveal melanoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Singh A.D., Seregard S., editors. Ocular Tumours. Volume 7. S. Karger AG; Basel, Switzerland: 2016. (ESASO Course Series).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
