

Understanding the Challenges and Uncertainties of Seroprevalence Studies for SARS-CoV-2
- PMID: 33925518
- PMCID: PMC8123865
- DOI: 10.3390/ijerph18094640
Understanding the Challenges and Uncertainties of Seroprevalence Studies for SARS-CoV-2
Abstract
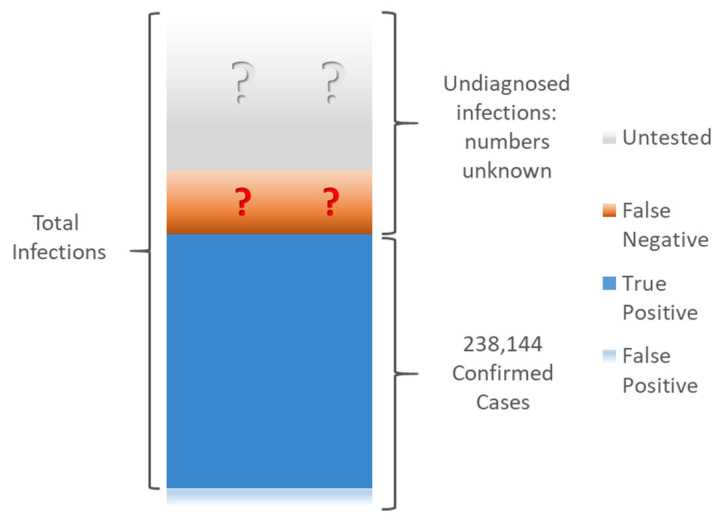
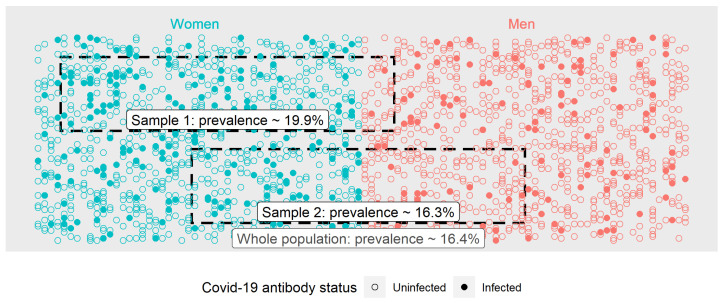
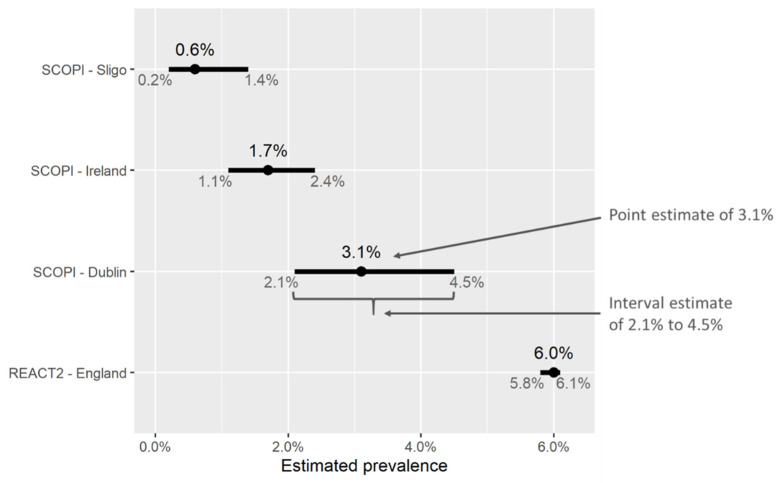
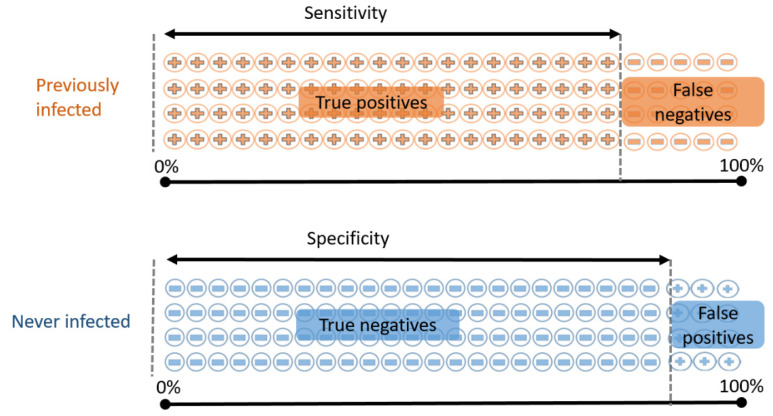
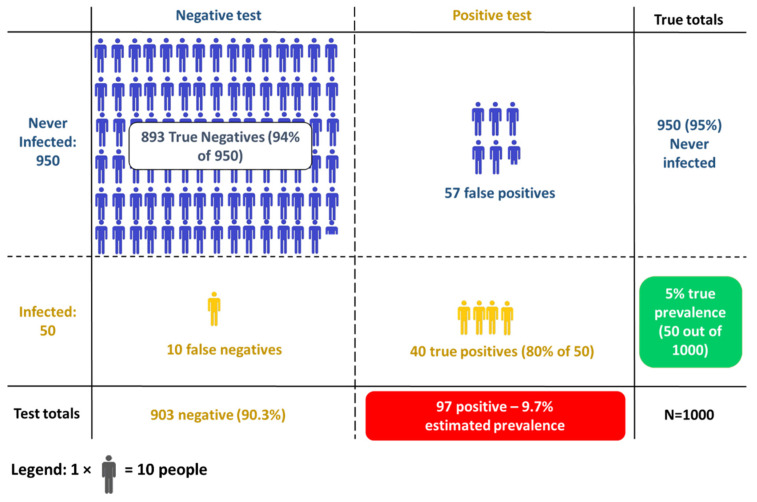
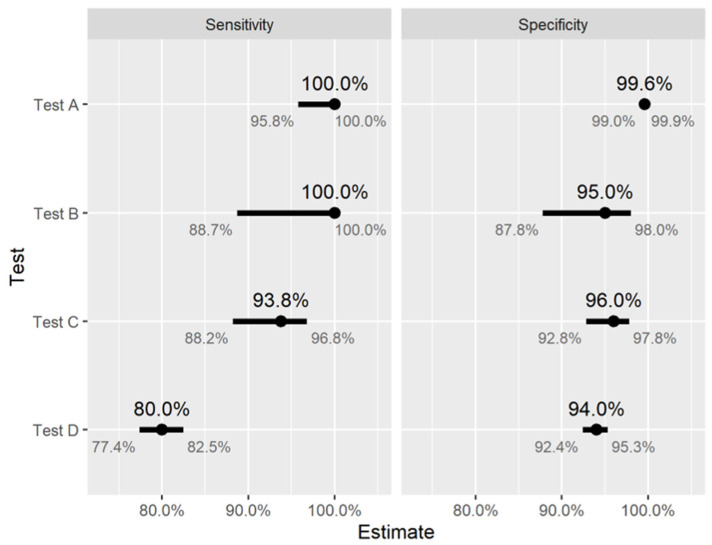
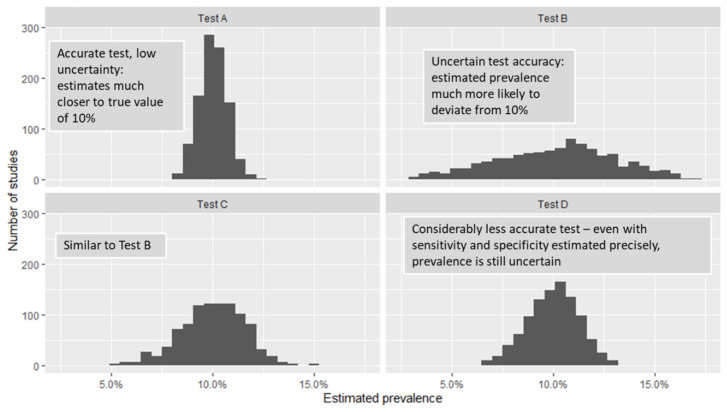
SARS-CoV-2 continues to widely circulate in populations globally. Underdetection is acknowledged and is problematic when attempting to capture the true prevalence. Seroprevalence studies, where blood samples from a population sample are tested for SARS-CoV-2 antibodies that react to the SARS-CoV-2 virus, are a common method for estimating the proportion of people previously infected with the virus in a given population. However, obtaining reliable estimates from seroprevalence studies is challenging for a number of reasons, and the uncertainty in the results is often overlooked by scientists, policy makers, and the media. This paper reviews the methodological issues that arise in designing these studies, and the main sources of uncertainty that affect the results. We discuss the choice of study population, recruitment of subjects, uncertainty surrounding the accuracy of antibody tests, and the relationship between antibodies and infection over time. Understanding these issues can help the reader to interpret and critically evaluate the results of seroprevalence studies.
Keywords: COVID-19; SARS-CoV-2; antibody testing; coronavirus; seroprevalence.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Havers F.P., Reed C., Lim T., Montgomery J.M., Klena J.D., Hall A.J., Fry A.M., Cannon D.L., Chiang C.-F., Gibbons A., et al. Seroprevalence of Antibodies to SARS-CoV-2 in 10 Sites in the United States, March 23–May 12, 2020. JAMA Intern. Med. 2020;180:1576–1586. doi: 10.1001/jamainternmed.2020.4130. - DOI - PMC - PubMed
-
- Russell T.W., Golding N., Hellewell J., Abbott S., Wright L., Pearson C.A.B., van Zandvoort K., Jarvis C.I., Gibbs H., Liu Y., et al. Reconstructing the Early Global Dynamics of Under-Ascertained COVID-19 Cases and Infections. BMC Med. 2020;18:332. doi: 10.1186/s12916-020-01790-9. - DOI - PMC - PubMed
-
- World Health Organisation Diagnostic Testing for SARS-CoV-2. [(accessed on 19 January 2021)]; Available online: https://www.who.int/publications-detail-redirect/diagnostic-testing-for-....
-
- European Centre for Disease Control Diagnostic Testing and Screening for SARS-CoV-2. [(accessed on 19 January 2021)]; Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/diagnostic-testing.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
