

Metabolic Spectrum of Liver Failure in Type 2 Diabetes and Obesity: From NAFLD to NASH to HCC
- PMID: 33925827
- PMCID: PMC8123490
- DOI: 10.3390/ijms22094495
Metabolic Spectrum of Liver Failure in Type 2 Diabetes and Obesity: From NAFLD to NASH to HCC
Abstract
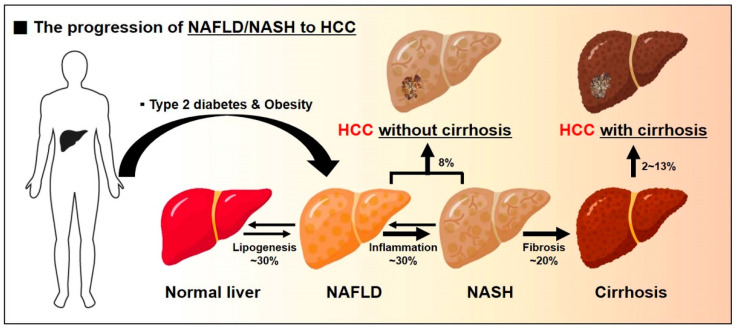
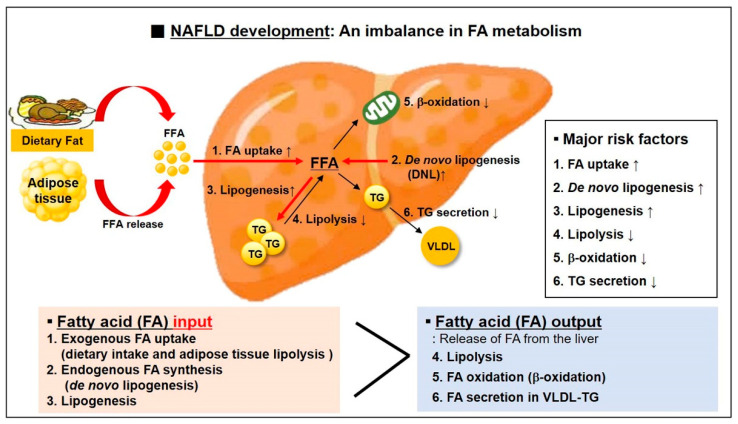
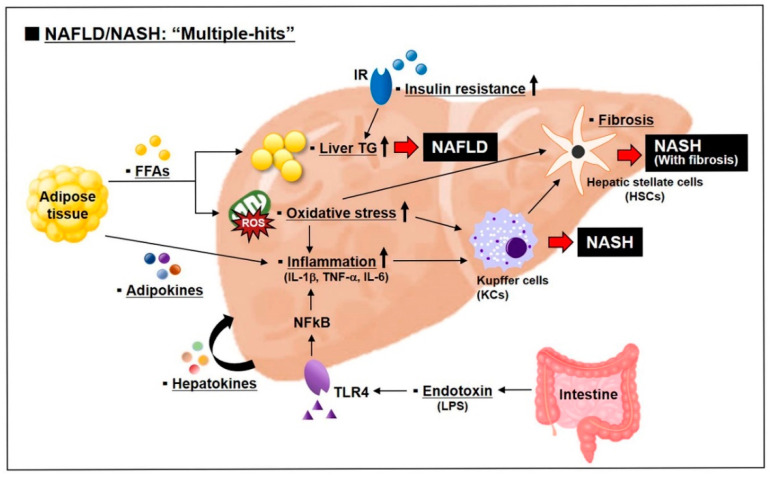
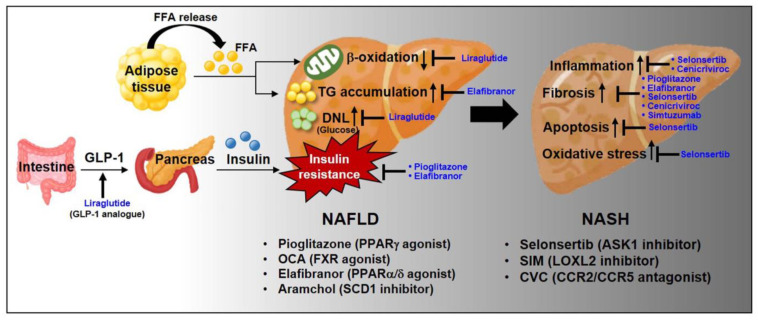
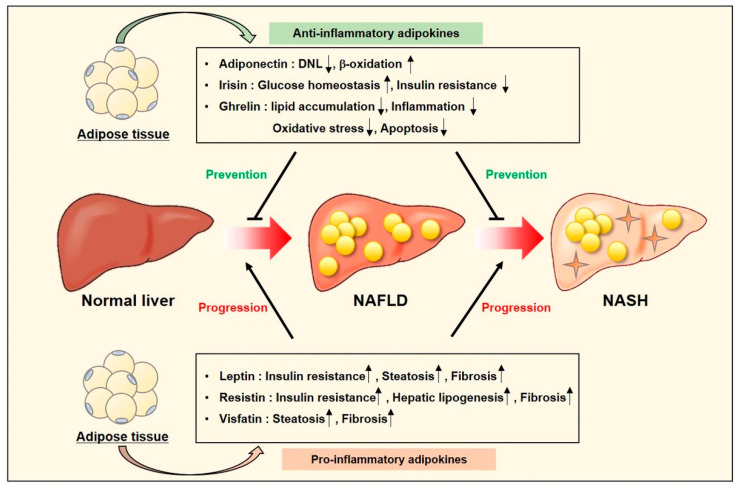
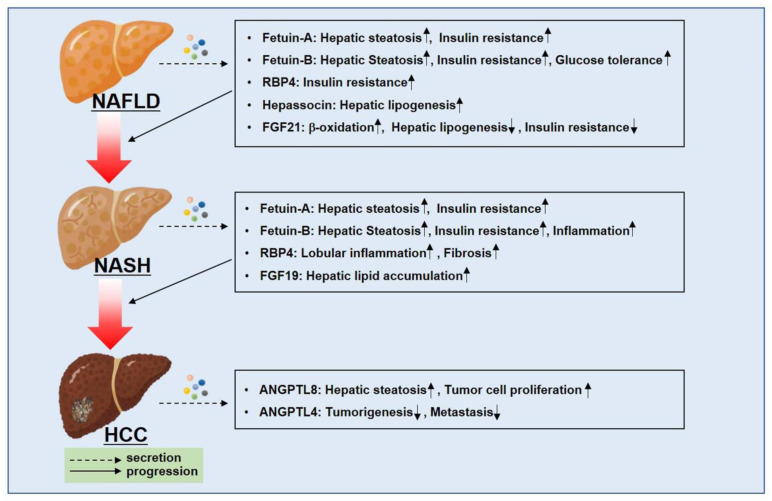
Liver disease is the spectrum of liver damage ranging from simple steatosis called as nonalcoholic fatty liver disease (NAFLD) to hepatocellular carcinoma (HCC). Clinically, NAFLD and type 2 diabetes coexist. Type 2 diabetes contributes to biological processes driving the severity of NAFLD, the primary cause for development of chronic liver diseases. In the last 20 years, the rate of non-viral NAFLD/NASH-derived HCC has been increasing rapidly. As there are currently no suitable drugs for treatment of NAFLD and NASH, a class of thiazolidinediones (TZDs) drugs for the treatment of type 2 diabetes is sometimes used to improve liver failure despite the risk of side effects. Therefore, diagnosis, prevention, and treatment of the development and progression of NAFLD and NASH are important issues. In this review, we will discuss the pathogenesis of NAFLD/NASH and NAFLD/NASH-derived HCC and the current promising pharmacological therapies of NAFLD/NASH. Further, we will provide insights into "adipose-derived adipokines" and "liver-derived hepatokines" as diagnostic and therapeutic targets from NAFLD to HCC.
Keywords: adipokines; hepatocellular carcinoma (HCC); hepatokines; non-alcholic fatty liver disease (NAFLD); non-alcoholic steatohepatitis (NASH); obesity; type 2 diabetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Satman I., Omer B., Tutuncu Y., Kalaca S., Gedik S., Dinccag N., Karsidag K., Genc S., Telci A., Canbaz B., et al. Twelve-year trends in the prevalence and risk factors of diabetes and prediabetes in Turkish adults. Eur. J. Epidemiol. 2013;28:169–180. doi: 10.1007/s10654-013-9771-5. - DOI - PMC - PubMed
-
- Masmiquel L., Leiter L.A., Vidal J., Bain S., Petrie J., Franek E., Raz I., Comlekci A., Jacob S., van Gaal L., et al. LEADER 5: Prevalence and cardiometabolic impact of obesity in cardiovascular high-risk patients with type 2 diabetes mellitus: Baseline global data from the LEADER trial. Cardiovasc. Diabetol. 2016;10:29. doi: 10.1186/s12933-016-0341-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
