

Advances in Targeting Cutaneous Melanoma
- PMID: 33925915
- PMCID: PMC8123429
- DOI: 10.3390/cancers13092090
Advances in Targeting Cutaneous Melanoma
Abstract
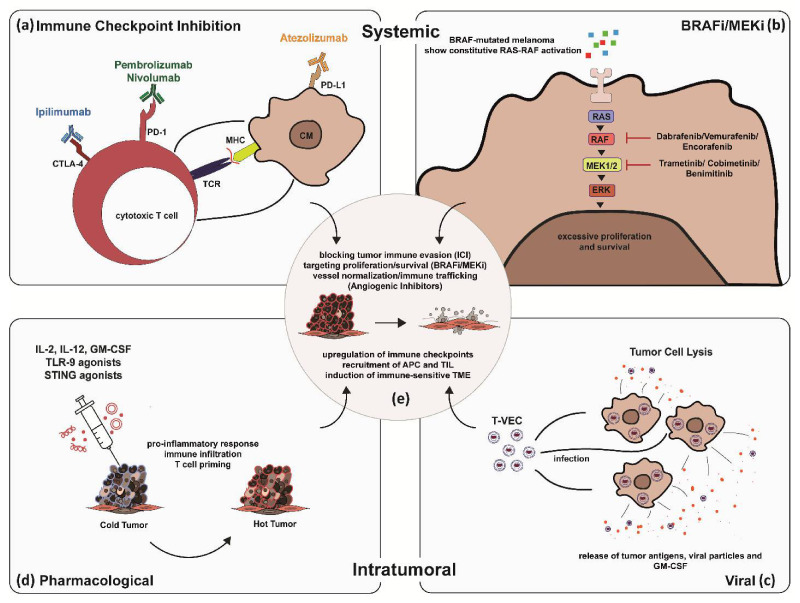
To date, the skin remains the most common cancer site among Caucasians in the western world. The complex, layered structure of human skin harbors a heterogenous population of specialized cells. Each cell type residing in the skin potentially gives rise to a variety of cancers, including non-melanoma skin cancer, sarcoma, and cutaneous melanoma. Cutaneous melanoma is known to exacerbate and metastasize if not detected at an early stage, with mutant melanomas tending to acquire treatment resistance over time. The intricacy of melanoma thus necessitates diverse and patient-centered targeted treatment options. In addition to classical treatment through surgical intervention and radio- or chemotherapy, several systemic and intratumoral immunomodulators, pharmacological agents (e.g., targeted therapies), and oncolytic viruses are trialed or have been recently approved. Moreover, utilizing combinations of immune checkpoint blockade with targeted, oncolytic, or anti-angiogenic approaches for patients with advanced disease progression are promising approaches currently under pre-clinical and clinical investigation. In this review, we summarize the current 'state-of-the-art' as well as discuss emerging agents and regimens in cutaneous melanoma treatment.
Keywords: cancer therapy; combination therapy; immunotherapy; intratumoral therapy; melanoma; skin cancer; targeted therapy.
Conflict of interest statement
L.S. has received speakers and/or advisory board honoraria from BMS, Sun-Pharma, MSD, and Novartis. T.G. has received speakers and/or advisory board honoraria from BMS, Sanofi-Genzyme, MSD, Novartis Pharma, Roche, Abbvie, Almirall, Janssen, Lilly, Pfizer, Pierre Fabre, Merck-Serono, outside the submitted work. D.K. and M.S. have no conflict of interest to declare.
Figures


References
-
- Skin Cancer Foundation Skin Cancer Facts and Statistics. Skin Cancer Information. Last Updated: January 13, 2021. [(accessed on 25 April 2021)]; Available online: https://www.skincancer.org/skin-cancer-information/skin-cancer-facts/
Publication types
LinkOut - more resources
Full Text Sources
