

Combination of Cyclosporine A and Levosimendan Induces Cardioprotection under Acute Hyperglycemia
- PMID: 33926009
- PMCID: PMC8123582
- DOI: 10.3390/ijms22094517
Combination of Cyclosporine A and Levosimendan Induces Cardioprotection under Acute Hyperglycemia
Abstract
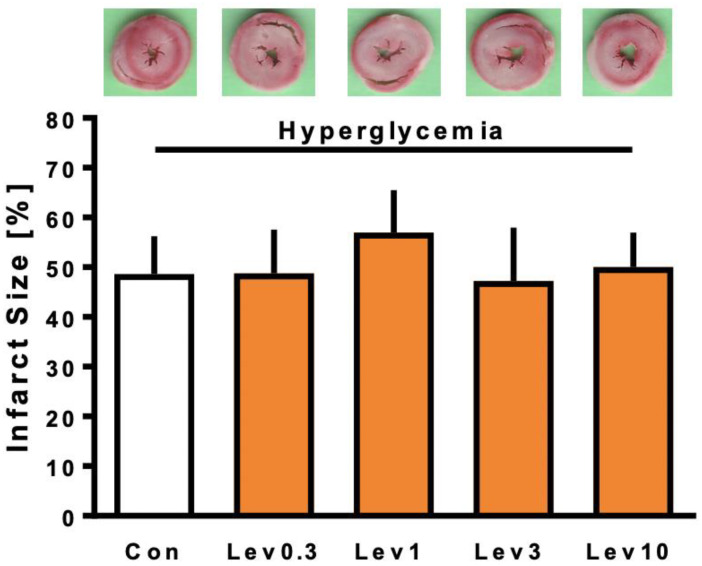
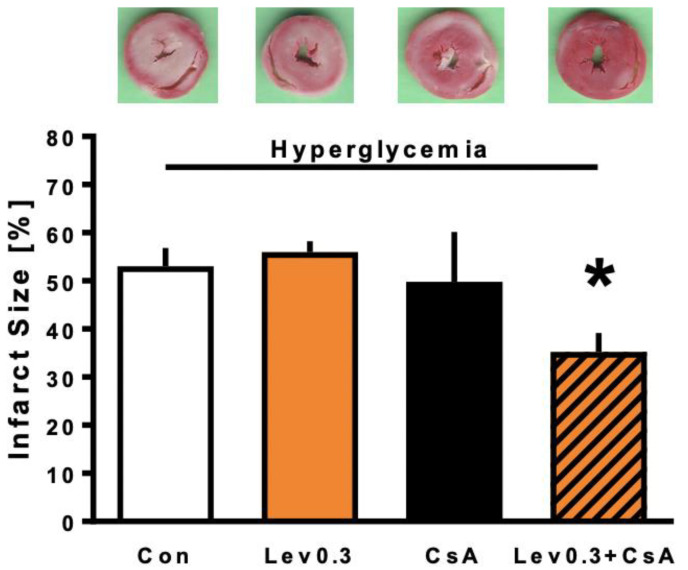
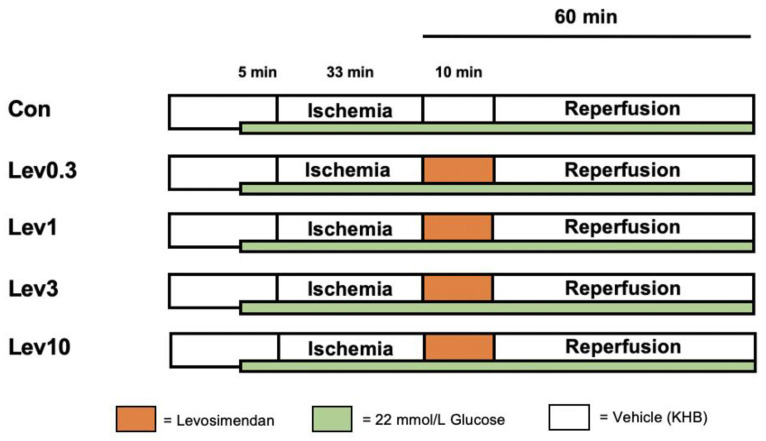
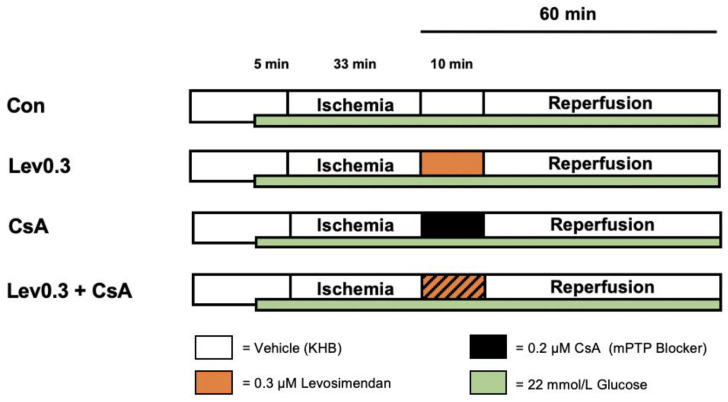
Prognosis of patients with myocardial infarction is detrimentally affected by comorbidities like diabetes mellitus. In the experimental setting, not only diabetes mellitus but also acute hyperglycemia is shown to hamper cardioprotective properties by multiple pharmacological agents. For Levosimendan-induced postconditioning, a strong infarct size reducing effect is demonstrated in healthy myocardium. However, acute hyperglycemia is suggested to block this protective effect. In the present study, we investigated whether (1) Levosimendan-induced postconditioning exerts a concentration-dependent effect under hyperglycemic conditions and (2) whether a combination with the mitochondrial permeability transition pore (mPTP) blocker cyclosporine A (CsA) restores the cardioprotective properties of Levosimendan under hyperglycemia. For this experimental investigation, hearts of male Wistar rats were randomized and mounted onto a Langendorff system, perfused with Krebs-Henseleit buffer with a constant pressure of 80 mmHg. All isolated hearts were subjected to 33 min of global ischemia and 60 min of reperfusion under hyperglycemic conditions. (1) Hearts were perfused with various concentrations of Levosimendan (Lev) (0.3-10 μM) for 10 min at the onset of reperfusion, in order to investigate a concentration-response relationship. In the second set of experiments (2), 0.3 μM Levosimendan was administered in combination with the mPTP blocker CsA, to elucidate the underlying mechanism of blocked cardioprotection under hyperglycemia. Infarct size was determined by tetrazolium chloride (TTC) staining. (1) Control (Con) hearts showed an infarct size of 52 ± 12%. None of the administered Levosimendan concentrations reduced the infarct size (Lev0.3: 49 ± 9%; Lev1: 57 ± 9%; Lev3: 47 ± 11%; Lev10: 50 ± 7%; all ns vs. Con). (2) Infarct size of Con and Lev0.3 hearts were 53 ± 4% and 56 ± 2%, respectively. CsA alone had no effect on infarct size (CsA: 50 ± 10%; ns vs. Con). The combination of Lev0.3 and CsA (Lev0.3 ± CsA) induced a significant infarct size reduction compared to Lev0.3 (Lev0.3+CsA: 35 ± 4%; p < 0.05 vs. Lev0.3). We demonstrated that (1) hyperglycemia blocks the infarct size reducing effects of Levosimendan-induced postconditioning and cannot be overcome by an increased concentration. (2) Furthermore, cardioprotection under hyperglycemia can be restored by combining Levosimendan and the mPTP blocker CsA.
Keywords: Levosimendan; cardioprotection; hyperglycemia; myocardial infarction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization The 10 Leading Causes of Death in the World, 2000 and 2012. [(accessed on 9 March 2021)]; Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
