

Spending on Cardiovascular Disease and Cardiovascular Risk Factors in the United States: 1996 to 2016
- PMID: 33926203
- PMCID: PMC8316421
- DOI: 10.1161/CIRCULATIONAHA.120.053216
Spending on Cardiovascular Disease and Cardiovascular Risk Factors in the United States: 1996 to 2016
Abstract
Background: Spending on cardiovascular disease and cardiovascular risk factors (cardiovascular spending) accounts for a significant portion of overall US health care spending. Our objective was to describe US adult cardiovascular spending patterns in 2016, changes from 1996 to 2016, and factors associated with changes over time.
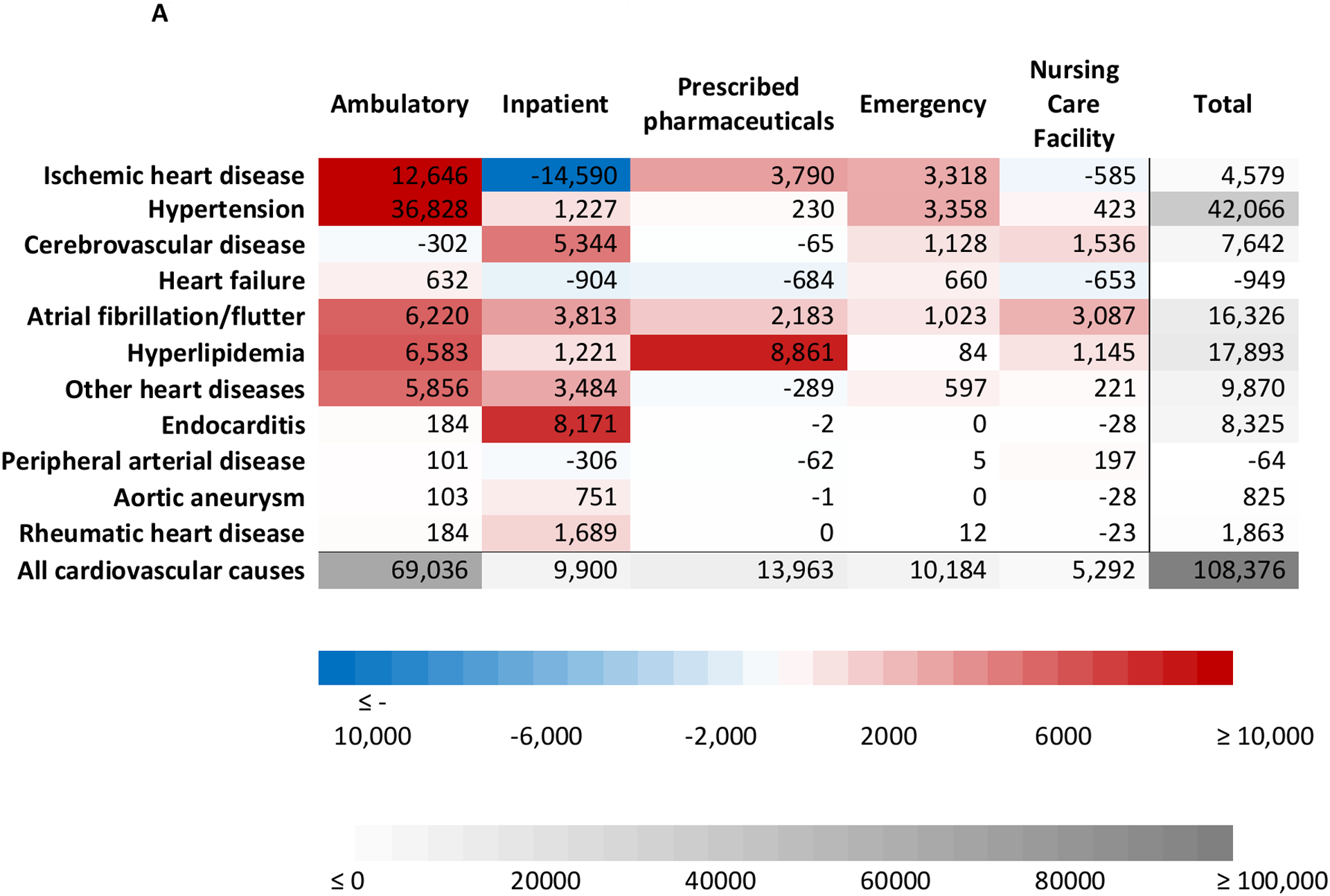
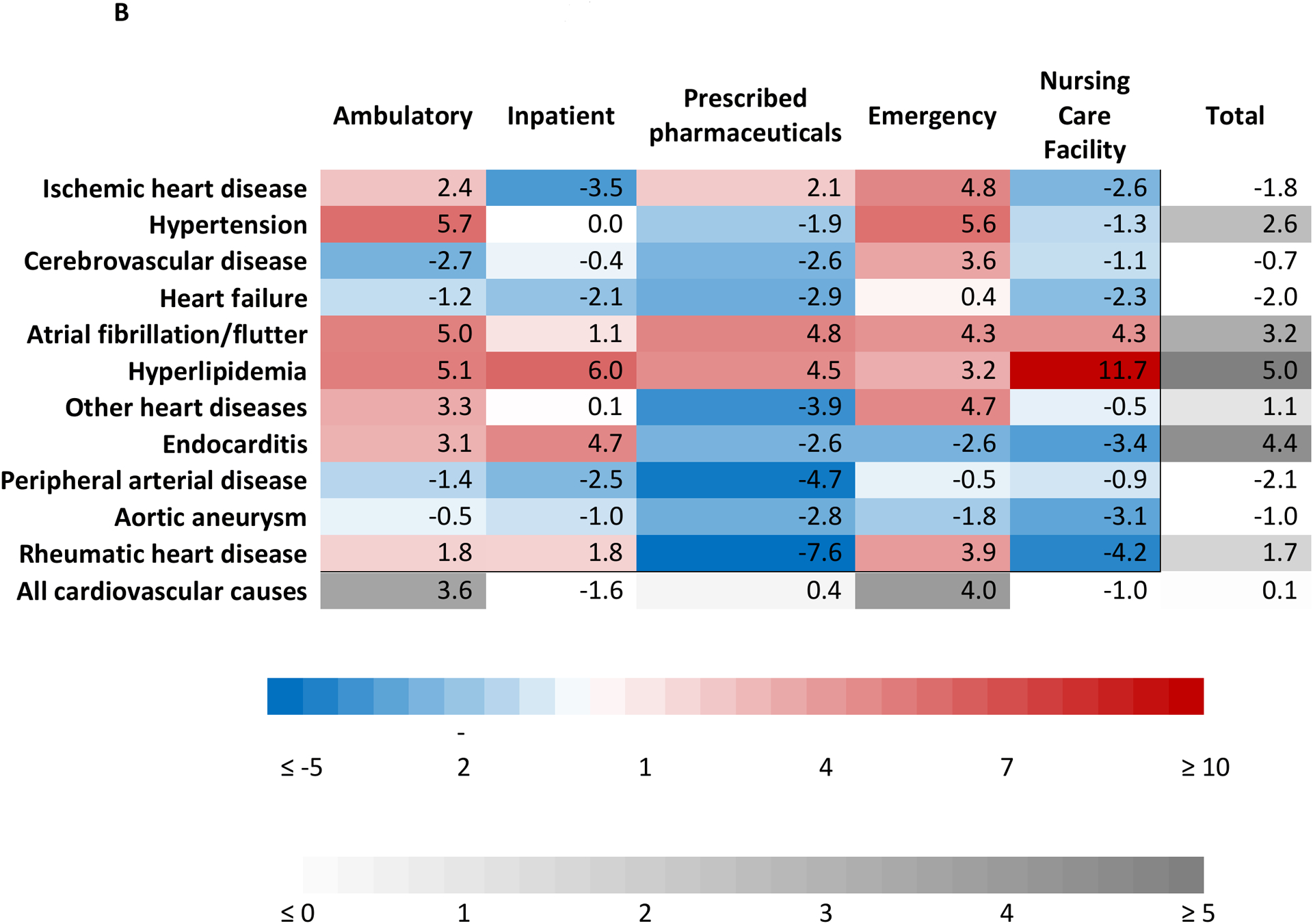
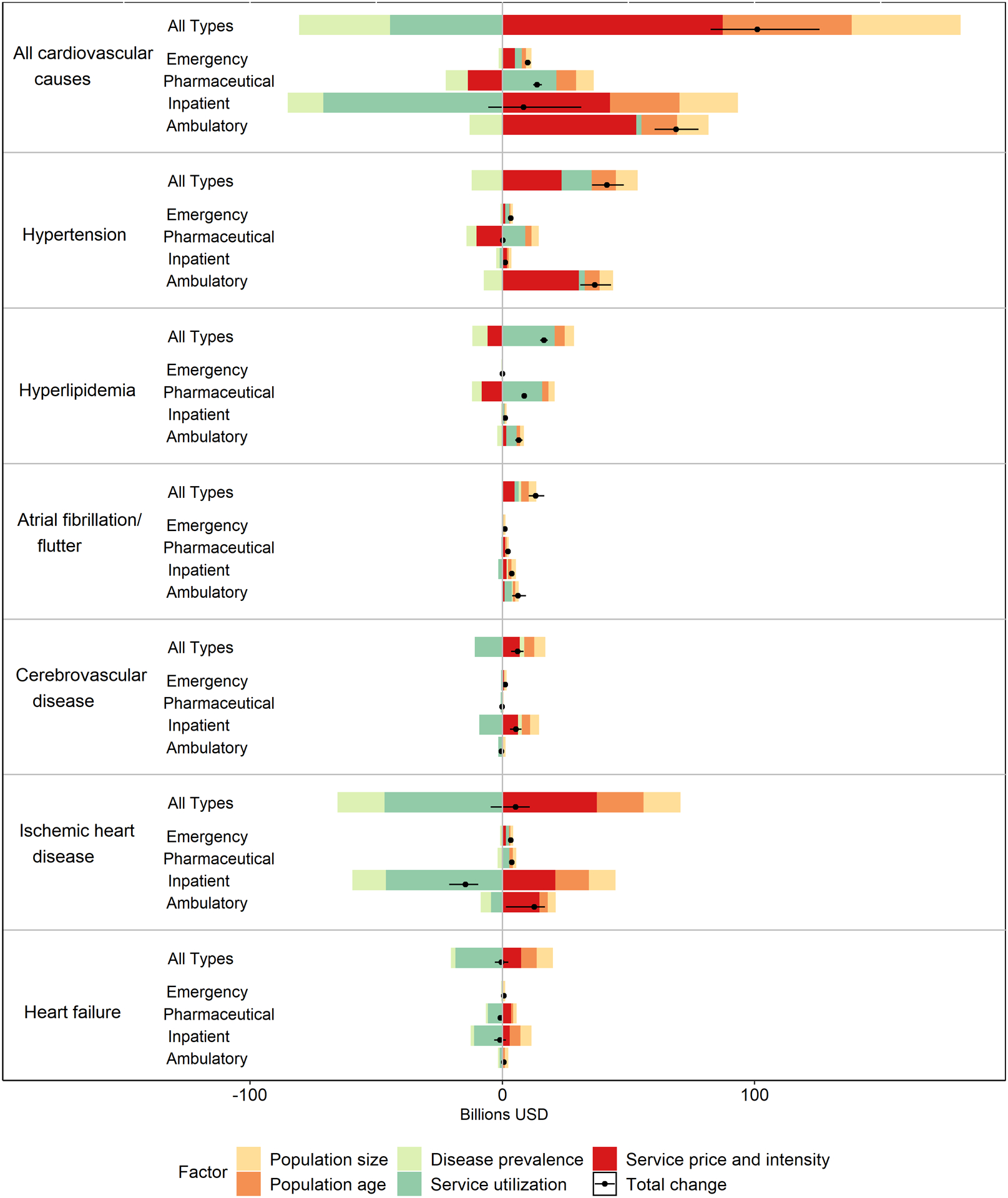
Methods: We extracted information on adult cardiovascular spending from the Institute for Health Metrics and Evaluation's disease expenditure project, which combines data on insurance claims, emergency department and ambulatory care visits, inpatient and nursing care facility stays, and drug prescriptions to estimate >85% of all US health care spending. Cardiovascular spending (2016 US dollars) was stratified by age, sex, type of care, payer, and cardiovascular cause. Time trend and decomposition analyses quantified contributions of epidemiology, service price and intensity (spending per unit of utilization, eg, spending per inpatient bed-day), and population growth and aging to the increase in cardiovascular spending from 1996 to 2016.
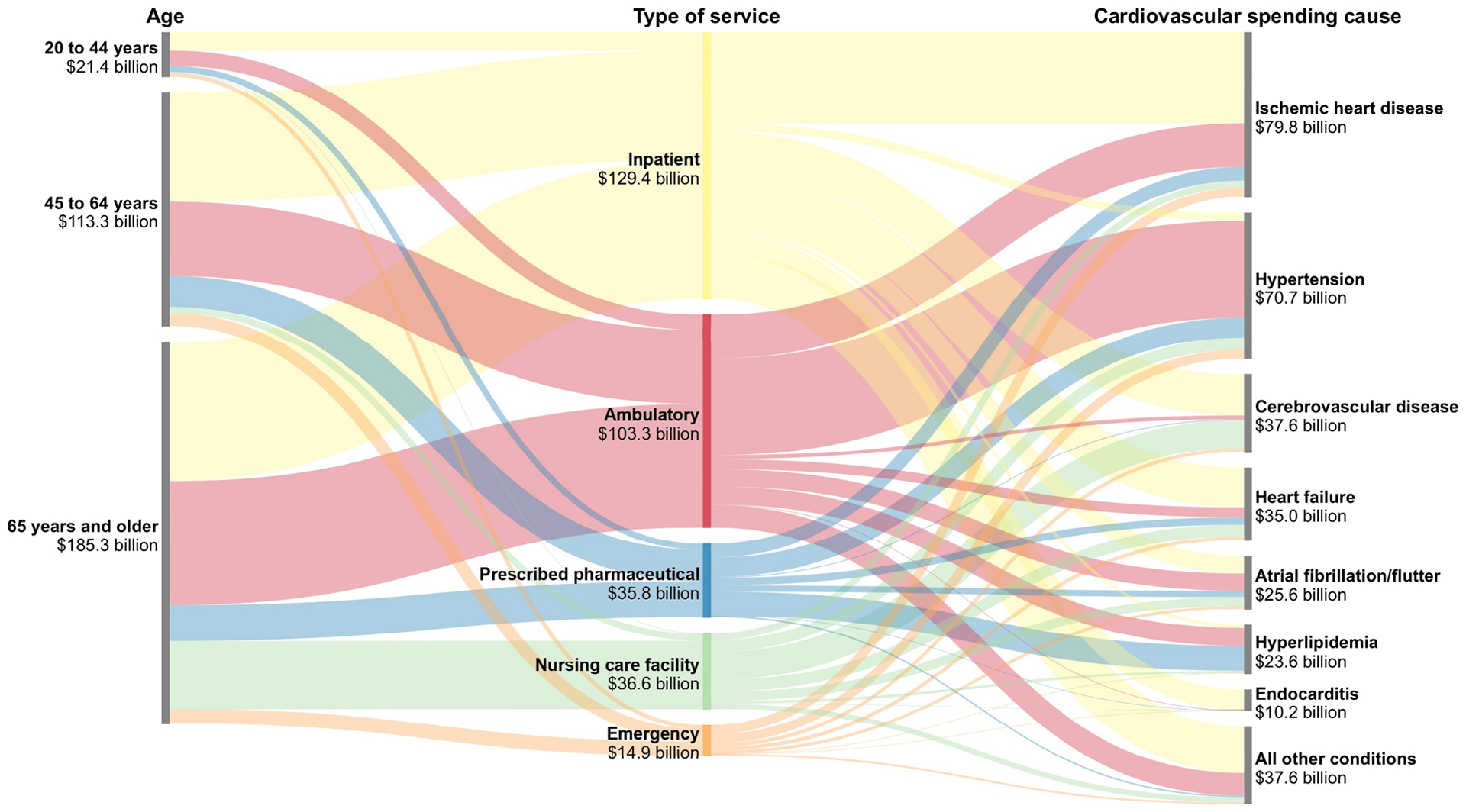
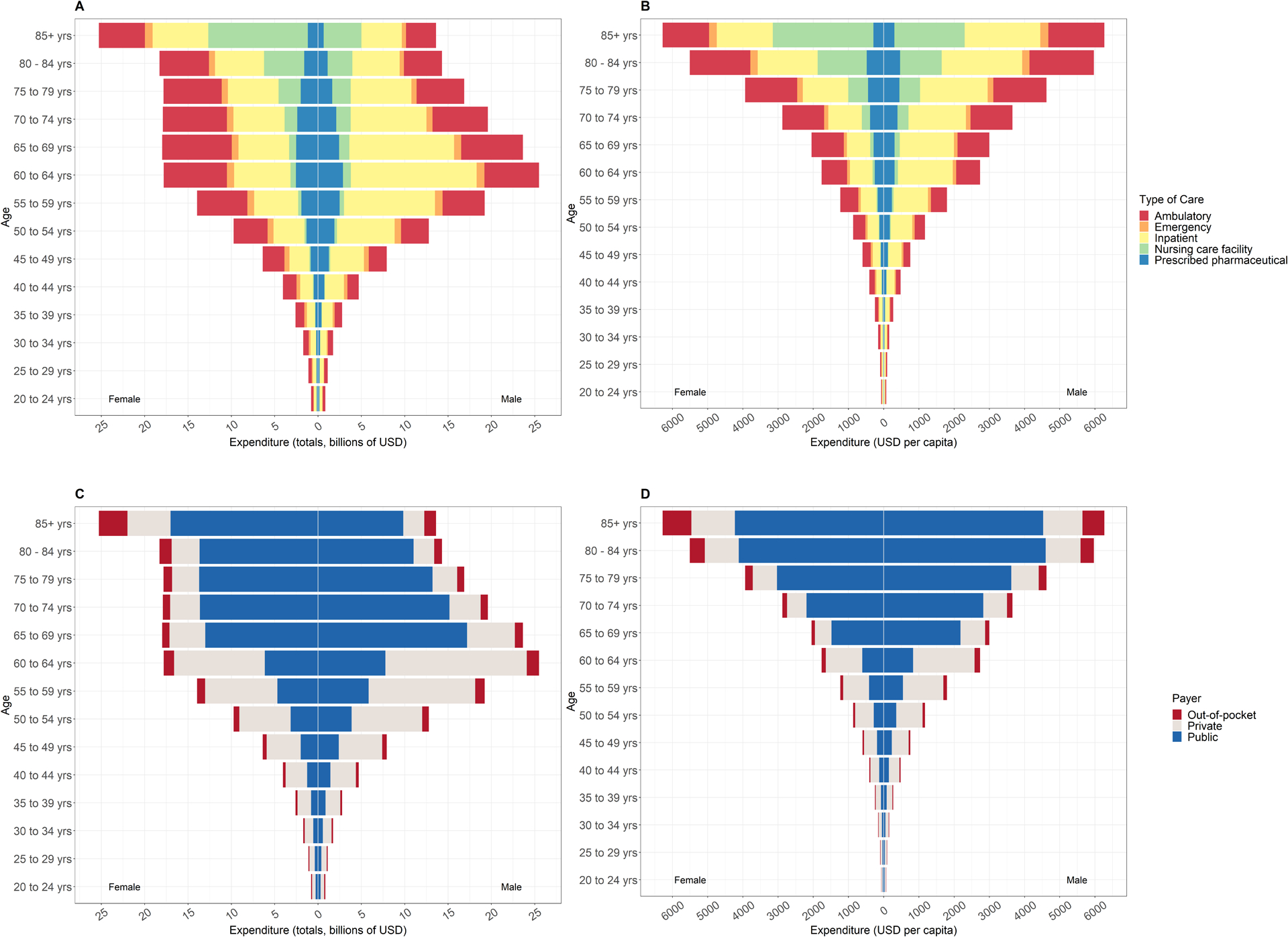
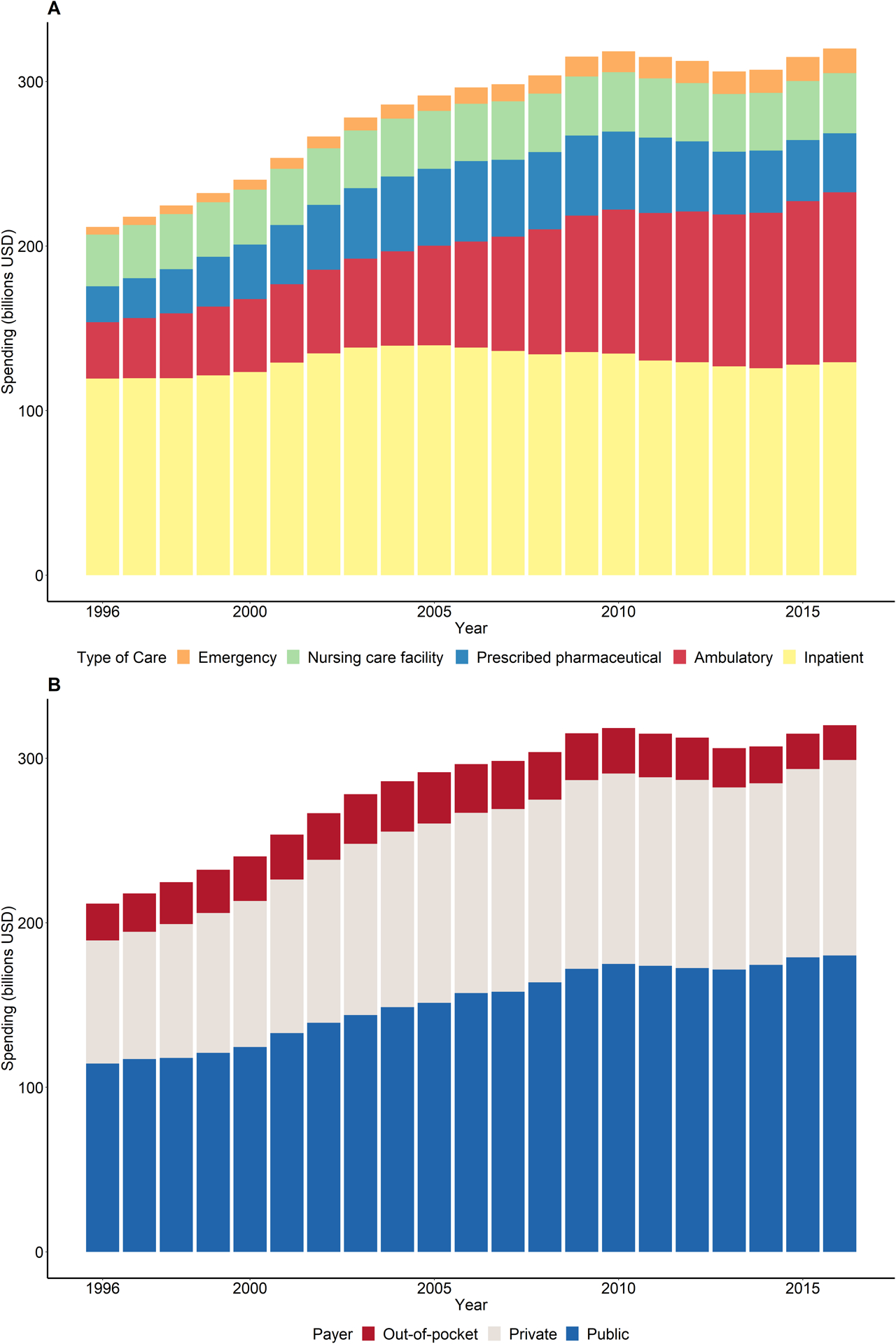
Results: Adult cardiovascular spending increased from $212 billion in 1996 to $320 billion in 2016, a period when the US population increased by >52 million people, and median age increased from 33.2 to 36.9 years. Over this period, public insurance was responsible for the majority of cardiovascular spending (54%), followed by private insurance (37%) and out-of-pocket spending (9%). Health services for ischemic heart disease ($80 billion) and hypertension ($71 billion) led to the most spending in 2016. Increased spending between 1996 and 2016 was primarily driven by treatment of hypertension, hyperlipidemia, and atrial fibrillation/flutter, for which spending rose by $42 billion, $18 billion, and $16 billion, respectively. Increasing service price and intensity alone were associated with a 51%, or $88 billion, cardiovascular spending increase from 1996 to 2016, whereas changes in disease prevalence were associated with a 37%, or $36 billion, spending reduction over the same period, after taking into account population growth and population aging.
Conclusions: US adult cardiovascular spending increased by >$100 billion from 1996 to 2016. Policies tailored to control service price and intensity and preferentially reimburse higher quality care could help counteract future spending increases caused by population aging and growth.
Keywords: cardiovascular; disease; health economics; health expenditures.
Conflict of interest statement
DISCLOSURES
All authors declare no relevant conflicts of interest to disclose.
Figures
Comment in
-
Is Rising Cardiovascular Spending a Good News or Bad News Story?Circulation. 2021 Jul 27;144(4):283-285. doi: 10.1161/CIRCULATIONAHA.121.055344. Epub 2021 Jul 26. Circulation. 2021. PMID: 34310163 No abstract available.
References
-
- Shah NS, Molsberry R, Rana JS, Sidney S, Capewell S, O’Flaherty M, Carnethon M, Lloyd-Jones DM, Khan SS. Heterogeneous trends in burden of heart disease mortality by subtypes in the United States, 1999–2018: observational analysis of vital statistics. BMJ. 2020;370:m2688. DOI: 10.1136/bmj.m2688. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
