

Blood Urea Nitrogen to Serum Albumin Ratio Independently Predicts Mortality in Critically Ill Patients With Acute Pulmonary Embolism
- PMID: 33926251
- PMCID: PMC8114751
- DOI: 10.1177/10760296211010241
Blood Urea Nitrogen to Serum Albumin Ratio Independently Predicts Mortality in Critically Ill Patients With Acute Pulmonary Embolism
Abstract
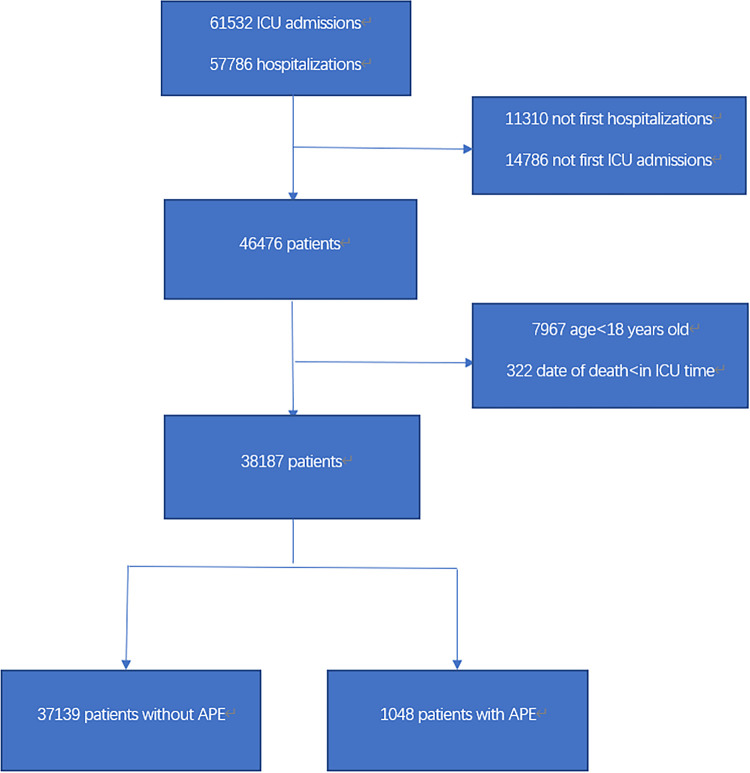
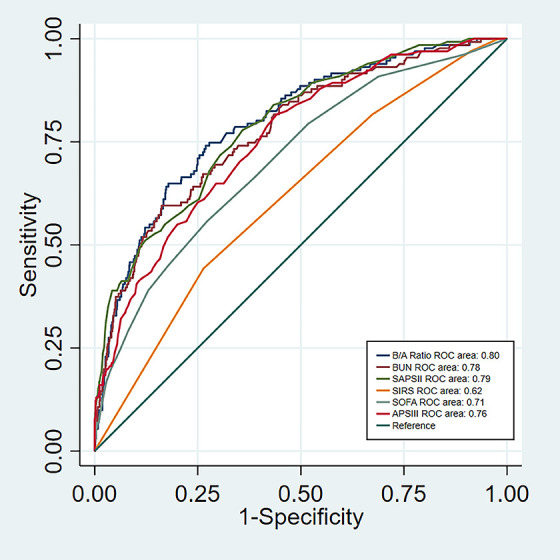
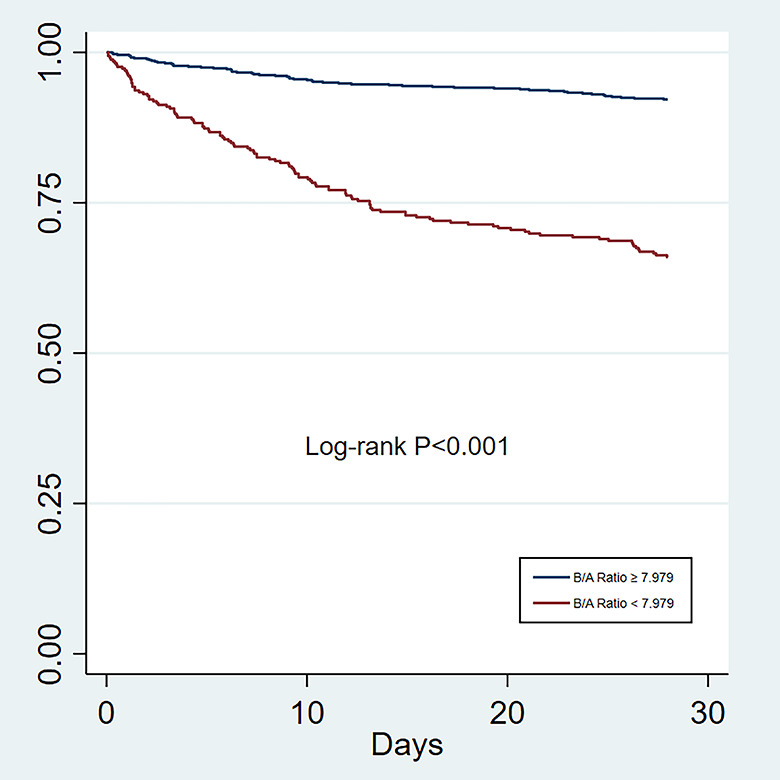
Acute pulmonary embolism (APE) is one of the prominent causes of death in patients with cardiovascular disease. Currently, reliable biomarkers to predict the prognosis of patients with APE are limited. The present study aimed to investigate the association of blood urea nitrogen to serum albumin (B/A) ratio and intensive care unit (ICU) mortality in critically ill patients with APE. A retrospective cohort study was performed using data extracted from a freely accessible critical care database (MIMIC-III). Adult (≥18 years) patients of first ICU admission with a primary diagnosis of APE in the database were enrolled in the study. The primary endpoint was the ICU mortality rate while the 28-day mortality after ICU admission was the secondary endpoint. The data of survivors and non-survivors were compared. A total of 1048 patients with APE were enrolled in this study, of which 131 patients died in ICU and 169 patients died within 28 days after ICU admission. The B/A ratio in the non-survivors group was significantly higher compared to the survivors group (P < 0.001). The multivariate analysis revealed that the B/A ratio was an independent predictor of ICU mortality (odds ratio [OR] 1.10, 95% CI 1.07-1.14, P < 0.001) and all-cause mortality within 28 days after ICU admission (hazard ratio [HR] 1.07, 95% CI 1.05-1.09, P < 0.001) in APE patients. The B/A ratio showed a greater area under the curve (AUC) of ICU mortality prediction (0.80; P < 0.001) than simplified acute physiology score II (SAPSII) (0.79), systemic inflammatory response syndrome score (SIRS) (0.62), acute physiology score III (APSIII) (0.76) and sequential organ failure assessment (SOFA) score (0.71). The B/A ratio could be a simple and useful prognostic tool to predict mortality in critically ill patients with APE.
Keywords: acute pulmonary embolism; blood urea nitrogen to serum albumin ratio; critical care; hospital mortality.
Conflict of interest statement
Figures
Similar articles
-
Synergistic impact of low serum albumin on intensive care unit admission and high blood urea nitrogen during intensive care unit stay on post-intensive care unit mortality in critically ill elderly patients requiring mechanical ventilation.Geriatr Gerontol Int. 2013 Jan;13(1):107-15. doi: 10.1111/j.1447-0594.2012.00869.x. Epub 2012 Jun 4. Geriatr Gerontol Int. 2013. PMID: 22672187
-
[Monocyte/lymphocyte ratio as a predictor of 30-day mortality and adverse events in critically ill patients: analysis of the MIMIC-III database].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 May;33(5):582-586. doi: 10.3760/cma.j.cn121430-20201223-00772. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 34112297 Chinese.
-
Predictive performance of blood urea nitrogen to serum albumin ratio in elderly patients with gastrointestinal bleeding.Am J Emerg Med. 2021 Mar;41:152-157. doi: 10.1016/j.ajem.2020.12.022. Epub 2020 Dec 23. Am J Emerg Med. 2021. PMID: 33465709
-
Systemic immune-inflammation index as a potential biomarker for predicting acute pulmonary embolism: A systematic review.Rom J Intern Med. 2024 Apr 9;62(3):231-240. doi: 10.2478/rjim-2024-0016. Print 2024 Sep 1. Rom J Intern Med. 2024. PMID: 38595041
-
Cardiooncology in the ICU - Cardiac Urgencies in Cancer Care.J Intensive Care Med. 2024 Dec 5:8850666241303461. doi: 10.1177/08850666241303461. Online ahead of print. J Intensive Care Med. 2024. PMID: 39632745 Review.
Cited by
-
Early prediction of mortality at sepsis diagnosis time in critically ill patients by using interpretable machine learning.J Clin Monit Comput. 2024 Apr;38(2):271-279. doi: 10.1007/s10877-023-01108-z. Epub 2023 Dec 27. J Clin Monit Comput. 2024. PMID: 38150124
-
Establishment and validation of a predictive nomogram for gestational diabetes mellitus during early pregnancy term: A retrospective study.Front Endocrinol (Lausanne). 2023 Feb 24;14:1087994. doi: 10.3389/fendo.2023.1087994. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 36909340 Free PMC article.
-
The correlation study between blood urea nitrogen to serum albumin ratio and prognosis of patients with sepsis during hospitalization.BMC Anesthesiol. 2022 Dec 28;22(1):404. doi: 10.1186/s12871-022-01947-4. BMC Anesthesiol. 2022. PMID: 36577937 Free PMC article.
-
Causal relationship between chronic kidney disease, renal function, and venous thromboembolism: a bidirectional Mendelian randomization study.Ren Fail. 2025 Dec;47(1):2496803. doi: 10.1080/0886022X.2025.2496803. Epub 2025 May 5. Ren Fail. 2025. PMID: 40321038 Free PMC article.
-
Association between blood-urea-nitrogen-to-albumin ratio and in-hospital mortality in patients diagnosed with coronavirus disease 2019: a retrospective cohort study.Eur J Med Res. 2025 Feb 4;30(1):78. doi: 10.1186/s40001-025-02338-4. Eur J Med Res. 2025. PMID: 39905533 Free PMC article.
References
-
- Konstantinides SV, Torbicki A, Agnelli G, et al. ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033–3080. doi:10.1093/eurheartj/ehu283 - PubMed
-
- Kucher N, Rossi E, De Rosa M, et al. Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med. 2005;165(15):1777–1781. doi:10.1001/archinte.165.15.1777 - PubMed
-
- Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronicthromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788–1830. doi:10.1161/CIR.0b013e318214914 f. - PubMed
-
- El-Menyar A, Sathian B, Al-Thani H. Elevated serum cardiac troponin and mortality in acute pulmonary embolism: Systematic review and meta-analysis. Respir Med. 2019;157: 26–35. doi:10.1016/j.rmed.2019.08.011 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
